Most people walk around completely oblivious to the fact that they might be harboring a tiny, thin-walled blister on a blood vessel in their head. It sits there, quiet and unassuming, until it isn't. The thing is, we tend to talk about medical emergencies as if they follow a predictable script, but the reality of a ruptured aneurysm is chaotic, messy, and terrifyingly fast. I believe we over-medicalize the description to the point where we lose the sheer, visceral horror of what is essentially a plumbing failure in the most expensive real estate of the human body. One minute you are reaching for a cup of coffee or laughing at a joke, and the next, your internal biology has declared war on your consciousness.
Understanding the Structural Vulnerability: Why Blood Vessels Fail Without Warning
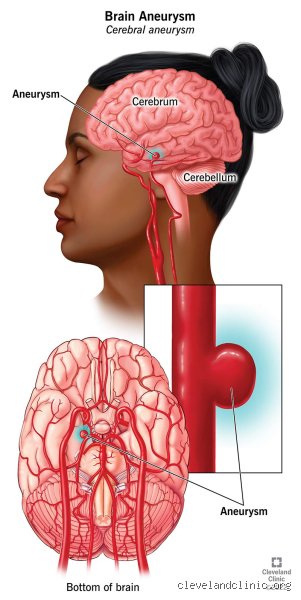
To grasp why these things pop, you have to look at the architecture of the Circle of Willis. This is a pentagonal circuit of arteries at the base of the brain where major vessels meet, and it’s a notorious hotspot for trouble because of the way fluid dynamics work. Think of it like a garden hose with a weak spot; over time, the constant thumping of blood—roughly 70 to 100 times per minute—stretches the vessel wall until it balloons out into a saccular shape. Doctors call these "berry" aneurysms because they dangle off the vessel like fruit on a stem, but that’s a bit too poetic for something that can kill you before you hit the floor. The issue remains that we still don't fully understand why some people have vessels made of tempered steel while others have arteries that give way under the slightest provocation of high blood pressure or genetic bad luck.
The Histology of a Weakness
The wall of a healthy artery is a three-layered masterpiece of smooth muscle and elastic fibers, but in an aneurysm, the middle layer—the tunica media—is often missing or severely thinned. Without that muscular reinforcement, the vessel relies on a translucent membrane of collagen to hold back the tide. When that membrane fails, blood enters the subarachnoid space at the same pressure it leaves the heart. This isn't a slow leak. It’s an explosion. Statistics from the Brain Aneurysm Foundation suggest that about 6.5 million people in the United States currently have an unruptured aneurysm, yet the vast majority will never know it unless they happen to get an MRI for an unrelated sinus headache or a minor car accident. We’re far from it being a routine screening, which is a frustrating reality of modern preventative medicine.
The Cascade of Chaos: The First Sixty Seconds of a Rupture
The moment the wall breaches, the brain is subjected to a dual-pronged assault: the loss of blood flow to downstream tissues and the crushing weight of the blood pooling in the skull. But here is where it gets tricky. People assume the "stroke" part is just about the bleeding, yet the sudden surge in intracranial pressure (ICP) can actually equal the systemic blood pressure for a few brief moments. When these two pressures equalize, blood stops flowing into the brain entirely. It is a literal standstill. This "transient global ischemia" is why so many victims lose consciousness immediately—their brain simply stalls because it cannot fight the internal pressure to get fresh oxygen. And if the pressure doesn't drop quickly? Then the brainstem, which controls your breathing and heart rate, gets pushed toward the opening at the base of the skull in a process called herniation.
The Chemical Firestorm in the Cerebrospinal Fluid
Blood is supposed to stay inside the pipes. When it escapes into the cerebrospinal fluid (CSF), it acts as a massive irritant. This isn't just about pressure; it's about chemistry. The breakdown of red blood cells releases oxyhemoglobin, which is toxic to the surrounding neural tissue and triggers a violent inflammatory response. You might think the body would have a better way to handle this, but it doesn't. Instead, the surrounding arteries react to this chemical insult by slamming shut—a secondary complication known as vasospasm. This typically happens days later, which explains why a patient can survive the initial burst only to suffer a massive stroke a week later while sitting in an ICU bed. It's a cruel irony that the body’s attempt to "clot" the leak often leads to starving the rest of the brain of nutrients.
The Role of Autonomic Storming
The hypothalamus, the brain's command center for the nervous system, sits right in the splash zone of a typical rupture. When it gets bathed in blood, it goes haywire. This leads to something called sympathetic storming, where the body is flooded with adrenaline and cortisol. Your heart rate might skyrocket, your blood pressure climbs even higher—further stressing the leak—and your lungs can even fill with fluid in a phenomenon called neurogenic pulmonary edema. In short, the brain’s distress signal causes the rest of the organs to panic, creating a systemic failure that complicates the efforts of even the most skilled neurosurgical teams. Is it any wonder that 40 percent of these events are fatal before the patient even reaches a hospital? Honesty is required here: sometimes the damage is so total, so immediate, that medicine is essentially a spectator.
The Triage of Symptoms: Identifying the Thunderclap Headache
We need to talk about the "Sentinel Leak." In about 15 to 60 percent of cases, patients experience a smaller, less severe headache in the days or weeks leading up to the big one. It’s a warning shot across the bow. Yet, because people are used to migraines or tension headaches, these warnings are frequently ignored or dismissed by primary care providers as mere stress. The distinction is the speed of onset. A migraine builds over an hour; a ruptured aneurysm peaks in less than a second. Imagine a lightning bolt hitting your neck and radiating up to your eyes. That changes everything. If you see someone grab their head and collapse, or if they complain of a stiff neck and sudden light sensitivity alongside that pain, the clock is already ticking against them.
Neurological Deficits and the Cranial Nerves
Beyond the pain, a bursting aneurysm often announces itself through the eyes. If the bulge is located on the posterior communicating artery, it can press against the third cranial nerve as it expands or leaks. As a result: one pupil might suddenly dilate and stay fixed, or an eyelid might droop. This is a neurosurgical emergency that demands an immediate CT scan. But wait, what if the symptoms are more subtle? Some people just feel "off" or experience a sudden bout of nausea and vomiting that looks like a stomach flu. Except that the nausea is accompanied by a neck so stiff they can't touch their chin to their chest. That rigidity is caused by blood irritating the meninges, the protective lining of the spinal cord, and it is a classic sign of meningeal irritation that should never be ignored.
Comparing Rupture Dynamics: Why Size Isn't the Only Factor
There is a prevailing myth in some clinical circles that only large aneurysms—those over 7 millimeters—are dangerous. This is a dangerous oversimplification. While it is true that larger "blisters" have higher wall tension according to Laplace’s Law, many ruptured aneurysms found in ERs are actually quite small, sometimes measuring only 3 or 4 millimeters. Why? Because the shape and the "aspect ratio" of the aneurysm matter just as much as the diameter. A small, irregular aneurysm with a "daughter sac" (a smaller bump on top of the main bulge) is often more unstable than a large, perfectly round one. We also have to consider the patient's lifestyle. A 2021 study showed that even a heavy lifting session or a bout of extreme anger can provide the final spike in blood pressure needed to tear a compromised vessel wall.
Genetics vs. Environment: Who is at Risk?
While we often blame lifestyle choices like smoking—which is the single most significant modifiable risk factor, increasing rupture risk by three to four times—genetics hold a heavy hand. Conditions like Ehlers-Danlos syndrome or polycystic kidney disease (PKD) create systemic weaknesses in connective tissue. If you have two first-degree relatives who have suffered a subarachnoid hemorrhage, your own risk jumps significantly. Yet, the nuance here is that most people who suffer a rupture have no known genetic markers. It’s a confluence of high blood pressure, perhaps a history of heavy alcohol use, and the sheer bad luck of having a vessel bifurcate at a sharp angle that catches the full force of the blood's kinetic energy. This unpredictability is what makes the condition so haunting for neurologists; you can manage the blood pressure, but you can’t change the plumbing you were born with.
The Mirage of the Minor Migraine: Common Mistakes and Misconceptions
Society loves a dramatic collapse, but the reality of a ruptured vessel is often far more insidious. Subarachnoid hemorrhage does not always announce itself with a theatrical faint; instead, the issue remains that many patients wait for a crescendo that never comes. The problem is that people equate "manageable" with "safe," ignoring the physiological tsunami occurring within their cranium. Because the initial leak might be microscopic, the body attempts a futile self-repair that masks the impending disaster. Let's be clear: a dull ache that transforms into a lightning strike is not a common headache, yet thousands of individuals treat it with over-the-counter ibuprofen while their neurological clock ticks toward zero.
The "Stroke Only Happens to the Elderly" Myth
Biological age is a deceptive metric when discussing arterial integrity. While degenerative wear-and-tear affects octogenarians, intracranial aneurysms frequently target the 35 to 60 age demographic with terrifying precision. Data suggests that approximately 40 percent of these catastrophic events occur in otherwise healthy, middle-aged adults, often those with a genetic predisposition or undiagnosed hypertension. It is a mistake to assume youth provides a bulletproof vest against vascular failure. A sudden, debilitating pain in a 40-year-old marathon runner is just as likely to be a bleed as it is in a sedentary retiree. We must stop associating brain bleeds exclusively with the nursing home; the fragility of the Circle of Willis is an equal-opportunity destroyer.
Mistaking the Sentinel Leak for Sinus Pressure
Around 15 to 60 percent of patients experience what experts call a sentinel headache days or weeks before a massive rupture. This is a warning shot across the bow. Except that most people dismiss these "warning leaks" as seasonal allergies or a stiff neck from a bad pillow. The issue remains that the medical community still sees patients arriving in the ER three days late, having ignored a sudden, sharp pain that dissipated quickly. By the time the secondary, catastrophic bleed occurs, the mortality rate spikes to nearly 50 percent. Do not wait for the "worst headache of your life" to become a permanent memory loss; even a strange, localized throb warrants a CTA scan to rule out a ticking time bomb.
The Vasospasm Paradox: The Invisible Second Wave
Surviving the initial burst is merely the prologue to a much grittier survival horror story. Once the blood exits the vessel and bathes the brain tissue, it acts as a toxic irritant. This leads to a phenomenon known as delayed cerebral ischemia or vasospasm, where the surrounding arteries constrict in a panicked, involuntary reaction to the spilled hemoglobin. It is a cruel irony that the brain’s response to a bleed is to starve itself of oxygen by squeezing its own pipes shut. Which explains why many patients seem "out of the woods" on day three, only to suffer a massive stroke on day seven (a terrifyingly common timeline in neuro-intensive care). (We often find ourselves fighting the body's own defense mechanisms more than the original injury.)
The Critical Window of Chemical Toxicity
Blood is life when it stays in the plumbing, but it is a neurotoxin when it touches the gray matter. As the red blood cells break down, they release free radicals and inflammatory cytokines that strip the protective coating from neurons. This chemical warfare usually peaks between day 4 and day 12 post-rupture. Physicians must utilize transcranial Doppler ultrasounds daily to monitor blood flow velocities, as a sudden spike indicates the vessels are narrowing to dangerous levels. In short, the "event" of an aneurysm bursting is not a single moment in time; it is a two-week marathon of metabolic instability that requires aggressive triple-H therapy—hypertension, hypervolemia, and hemodilution—to keep the brain perfused. Expert advice dictates that the real battle for neurological recovery begins only after the neurosurgeon has successfully clipped or coiled the source.
Frequently Asked Questions
What are the statistical chances of surviving a ruptured brain aneurysm?
The numbers are sobering and demand immediate attention. Statistics indicate that approximately 25 percent of individuals do not survive the initial 24 hours following the hemorrhagic event. Of those who reach the hospital alive, roughly 50 percent will succumb to complications within the first thirty days. As a result: only about one-third of survivors return to their baseline level of functioning without permanent cognitive deficits. These figures highlight that speed of intervention is the only variable we can truly control in a landscape of biological chaos.
Can stress or physical exertion cause an aneurysm to burst?
While an aneurysm is a structural defect present for years, a sudden spike in transmural pressure can act as the final straw. Activities involving heavy lifting, intense emotional outbursts, or even straining on the toilet can increase intracranial pressure enough to trigger a rupture in a weakened vessel wall. But is it the stress itself, or the underlying high blood pressure that does the damage? Most clinical evidence suggests that chronic, untreated hypertension is the primary driver, while the physical exertion is merely the immediate catalyst. Maintenance of a steady, low-pressure cardiovascular system remains the best defense against a sudden catastrophic failure.
What is the difference between clipping and coiling treatments?
The choice between these two interventions depends entirely on the aneurysm morphology and its location within the brain. Clipping is a traditional "open" surgery involving a craniotomy where a small metal clip is placed at the neck of the bulge to stop blood flow. Coiling is an endovascular procedure where a catheter is threaded from the groin to the brain to pack the aneurysm with platinum wires, inducing a clot. Studies like the International Subarachnoid Aneurysm Trial (ISAT) suggest coiling may have better short-term outcomes, yet clipping often provides a more definitive, long-term vascular seal. In short, the surgeon must decide between the invasiveness of a saw and the precision of a wire based on the patient's unique anatomy.
Beyond the Bleed: A Perspective on Proactive Vigilance
Modern medicine has turned a once-guaranteed death sentence into a survivable crisis, but we are far from conquering the cerebral aneurysm. The stance I take is firm: the current "wait and see" approach for small, unruptured bulges is a gamble with stakes no human should be asked to cover. We prioritize reactionary heroics over the mundane, expensive reality of preventative screening for high-risk families. It is an absurdity that we treat the brain as a black box until it starts leaking onto the floor. If you have a family history or persistent, localized neurological "oddities," demand a non-invasive MRA. Let's be clear: the only thing more expensive than an early scan is the lifelong cost of a hemorrhagic stroke. We must shift our cultural fear from the surgery to the silence of the undiagnosed vessel.