The Anatomy of Vulnerability: What Does It Actually Mean to Have an At-Risk Pancreas?
Think of your pancreas as an introverted powerhouse sitting quietly behind your stomach. It manufactures some of the most corrosive digestive enzymes in the human repository, including trypsinogen and lipase. Usually, these chemical weapons remain dormant until they travel down the pancreatic duct and hit the duodenum. But when the organ becomes structurally or metabolically compromised, everything breaks down. Premature enzyme activation occurs inside the acinar cells. Essentially, the organ begins to digest itself from the inside out, triggering a cascade of necrosis, localized edema, and systemic inflammatory response syndrome.
The Acute Versus Chronic Divergence
People often conflate the two manifestations, which is a dangerous clinical oversight. Acute pancreatitis is a sudden, violent volcanic eruption. One day you are fine, and the next you are curled in a fetal position in an emergency department room at Mount Sinai Hospital with agonizing pain radiating to your back. Chronic pancreatitis, conversely, is a slow, smoldering burn that quietly destroys healthy tissue over decades, replacing it with useless fibrotic scar tissue. Can you have one without the other? Mostly yes, but a severe acute episode can easily lay the groundwork for long-term tissue degradation, meaning the line between them is far more porous than traditional textbooks suggest.
The Diagnostic Blindspot That Sneaks Up on Clinicians
Where it gets tricky is that early-stage pancreatic insufficiency behaves like a chameleon. It mimics standard irritable bowel syndrome or gallbladder sludge, meaning early warning signs are routinely shrugged off. Doctors often rely too heavily on serum amylase and lipase spikes, yet in chronic cases or late-stage acute necrosis, those enzyme levels can actually appear totally normal because the tissue is too exhausted to produce them. It is a terrifying paradox.
The Two Titans of Risk: Gallstones and Ethanol Intake
Look at any global epidemiological study from the past half-century—whether it is from the Karolinska Institute in Sweden or a urban clinic in downtown Chicago—and you will find that mechanical obstruction and chemical toxicity cause roughly 75% of all documented cases. They are the twin engines of pancreatic disaster.
The Biliary Blockage Catastrophe
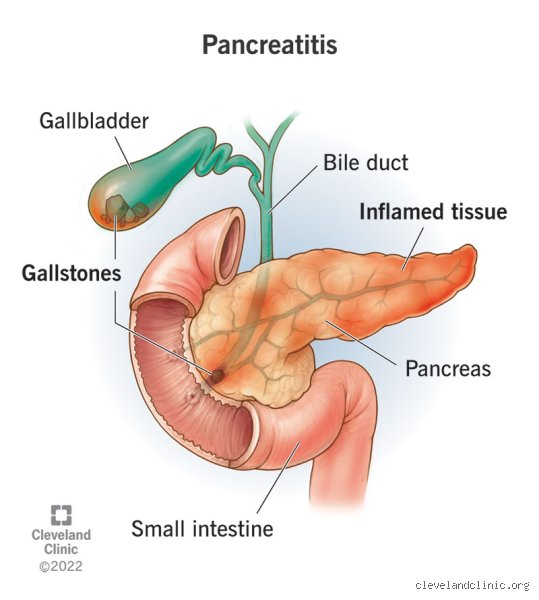
Gallstones are the absolute leading cause of acute pancreatitis worldwide. If you have a gallbladder packed with cholesterol or pigment stones, you are playing a high-stakes game of anatomical roulette. When a stone slips out of the gallbladder, it journeys down the common bile duct. But right before it empties into the small intestine, it encounters a narrow bottleneck called the Ampulla of Vater. If a stone gets wedged there, it blocks the pancreatic duct. The result? Pancreatic juices back up, pressure builds exponentially within the lumens, and the digestive enzymes go rogue. A tiny, three-millimeter gallstone can trigger a multi-week stay in an intensive care unit. Women over forty who meet certain metabolic criteria are statistically the primary targets here, a reality that changes everything when triaging abdominal pain.
The Alcohol Threshold Mystery
Then we have ethanol. For years, the prevailing medical narrative was that only severe, skid-row alcoholics developed pancreatic damage. We are far from it. While chronic consumption of more than four to five drinks per day over five years drastically elevates your risk profile, binge drinking can trigger an acute strike out of nowhere. How alcohol alters the pancreas is complex: it increases the permeability of ductules, makes pancreatic secretions incredibly thick and plug-like, and generates highly toxic metabolites like acetaldehyde within the acinar cells themselves. Yet, honestly, it's unclear why only about 10% of heavy drinkers ever develop clinical pancreatitis. There is an invisible, underlying genetic fuse that needs to be lit, which explains why your heavy-drinking neighbor might escape unscathed while someone else suffers organ failure after a holiday weekend benders.
Beyond the Usual Suspects: The Metabolic and Pharmaceutical Wildcards
If you don't drink and your gallbladder is clean, you might think you are entirely safe from this nightmare. You aren't. There is a whole underbelly of modern health crises driving pancreatic admissions across suburban hospitals right now.
The Lipid Crisis and the 1000 mg/dL Threshold
People don't think about this enough, but hypertriglyceridemia is a massive, aggressive trigger. If your fasting serum triglycerides climb above 1,000 milligrams per deciliter, your risk of acute pancreatic inflammation skyrockets exponentially. What happens is that excess circulating lipids are broken down by localized lipase into toxic, free fatty acids. These acids brutally damage the delicate capillary beds of the pancreas, inducing ischemia. I have seen patients who eat seemingly healthy diets but possess underlying genetic lipid disorders—like familial chylomicronemia syndrome—wind up with severe necrotizing disease. It is a stark reminder that outward appearance means nothing when your blood chemistry is sludge.
The Medication Traps Hidden in Plain Sight
Did you know your medicine cabinet could be a liability? Drug-induced pancreatitis accounts for up to 5% of cases, and the list of culprits is shockingly mundane. Common diuretics like furosemide, immunosuppressants like azathioprine, and even certain antibiotics like tetracycline can accidentally irritate the tissue. But the real discussion today centers around GLP-1 receptor agonists used for weight loss and type 2 diabetes. While the absolute risk remains low, post-marketing surveillance data has forced regulatory bodies to slap warnings on these blockbuster drugs. It makes sense—if you radically alter incretin kinetics and gastric emptying, the pancreas is inevitably going to feel the physiological ripple effects.
A Comparative Look at Genetic Vulnerability Versus Lifestyle Triggers
Is your fate written in your DNA, or is it forged at the dinner table? It is the classic nature versus nurture debate, but played out in the retroperitoneal space with incredibly high stakes.
The PRSS1 and SPINK1 Genetic Mutations
For a small segment of the population, lifestyle modifications are practically irrelevant because their genetic code has rigged the game against them. Mutations in the PRSS1 gene, which encodes cationic trypsinogen, essentially remove the "off switch" from digestive enzymes. If a tiny amount of trypsin activates prematurely inside the pancreas of a patient carrying this mutation, it cannot be deactivated. It triggers a domino effect of self-destruction. Another culprit is the SPINK1 mutation, which weakens the body's natural trypsin inhibitor shield. Patients with these hereditary mutations often experience their first agonizing bout of pancreatitis before the age of twenty, facing a lifetime risk of pancreatic adenocarcinoma that is 40% higher than the general public. For them, a single mistake in diet or hydration can mean immediate hospitalization.
Why Lifestyle Can Override or Amplify Genetic Fault Lines
But for the rest of us, lifestyle is the master thermostat that turns these risks up or down. Consider the impact of cigarette smoking. Everyone knows smoking destroys the lungs, but few realize it accelerates pancreatic calcification and fibrosis at an alarming rate. In fact, a smoker with a minor genetic predisposition to inflammation is nearly three times more likely to progress to chronic organ failure than a non-smoker with the exact same genetic profile. The issue remains that we live in a society that treats organs in isolation, ignoring how a puff of a cigarette in the lungs can alter the pH of secretions deep within the abdomen.
Common mistakes and dangerous misconceptions
The myth of the absolute teetotaler safety net
Think staying completely away from spirits grants you permanent immunity? Think again. The public consciousness routinely paints this condition as the exclusive punishment of chronic alcoholism, which explains why so many non-drinkers ignore the warning signs until emergency surgery becomes unavoidable. Biliary sludge and silent gallstones trigger a massive percentage of acute episodes, completely independent of your Friday night habits. Let's be clear: a perfectly sober lifestyle cannot shield an individual whose gallbladder is secretly manufacturing microscopic stones. When one of these calcified pebbles slips down and plugs the pancreatic duct, the organ begins digesting itself within hours. Consequently, assuming you are safe just because your bar cart is empty remains a perilous gamble.
Is it just a bad case of indigestion?
You feel a sharp, boring ache after a heavy meal. You reach for an antacid, expecting a quick burp and sudden relief, except that the fire in your upper abdomen refuses to die down. This is where misdiagnosis turns lethal. People routinely mistake the early, agonizing onset of pancreatic inflammation for basic acid reflux or a temporary food intolerance. Why do we minimize internal catastrophes? Because admitting your gut is failing feels far more terrifying than blaming a greasy taco. Waiting out the storm with over-the-counter chalk tablets allows enzymatic destruction to accelerate unchecked, turning a highly treatable localized swelling into a systemic inflammatory response that can compromise your lungs.
The false security of normal bloodwork
Medical statistics prove that standard lab panels can occasionally lie to your face. Some patients walk out of clinics reassured by standard liver enzymes, unaware that who is prone to pancreatitis cannot always be determined by a single routine blood draw. Chronic variations of the disease frequently exhibit entirely normal amylase levels because the scarred tissue has simply given up on producing enzymes altogether. Relying solely on basic screening tools creates a deceptive sense of calm, yet the underlying destruction continues its silent march toward permanent organ failure.
The hidden genetic clock and targeted expert intervention
Unmasking the PRSS1 mutant variant
Sometimes, the enemy lives directly inside your double helix. While lifestyle factors dominate the headlines, hereditary pancreatitis mutations like the PRSS1 or SPINK1 variants operate as ticking time bombs. If your family tree features multiple generations plagued by vague abdominal agony, you might possess an inherent structural flaw where trypsinogen activates prematurely inside the tissue. What can a clinical specialist actually do about a genetic destiny? The issue remains that we cannot rewrite your DNA, but we can radically alter your survival odds through aggressive, proactive monitoring.
The proactive protocol for high-risk profiles
We must pivot toward regular endoscopic ultrasounds and strict lipid management before the first flare-up strikes. If your fasting triglycerides regularly rocket past 500 milligrams per deciliter, you are standing on a trapdoor. Expert intervention means deploying fibric acid derivatives and specialized plasmapheresis to mechanically skim the thick fat from your bloodstream. It is not about waiting for the agony to start; it is about starving the trigger mechanisms before they pull themselves.
Frequently Asked Questions
Can a single night of binge drinking trigger a sudden acute attack?
Absolutely, because a sudden massive influx of ethanol forces the acinar cells to synthesize toxic metabolic byproducts at an unsustainable velocity. Clinical data indicates that consuming over 80 grams of pure alcohol in one sitting (roughly equivalent to five or six standard drinks) drastically spikes the pressure within the pancreatic ductal system. This acute toxicity causes the premature intracellular activation of digestive enzymes, which immediately begin destroying localized tissue. As a result, individuals with no prior history of gastrointestinal illness can find themselves in an intensive care unit within 24 hours of a celebratory party. Studies show that approximately 10% of acute cases are traced back to these isolated, high-volume sessions.
How exactly does a high-fat keto diet influence pancreatic vulnerability?
Forcing the body into