Let's be completely honest here: most people treat bleeding gums as a minor annoyance, akin to a paper cut, rather than a smoldering bacterial wildfire. We live in an era of hyper-advanced dentistry, yet 47.2% of adults aged 30 and older in the United States suffer from some form of periodontal disease, according to data from the Centers for Disease Control and Prevention (CDC). That is nearly half the adult population walking around with eroding jawbones. It makes you wonder why a condition so easily detectable remains a leading cause of adult tooth loss worldwide.
The Anatomy of Decline: Defining the Boundaries of Periodontal Health
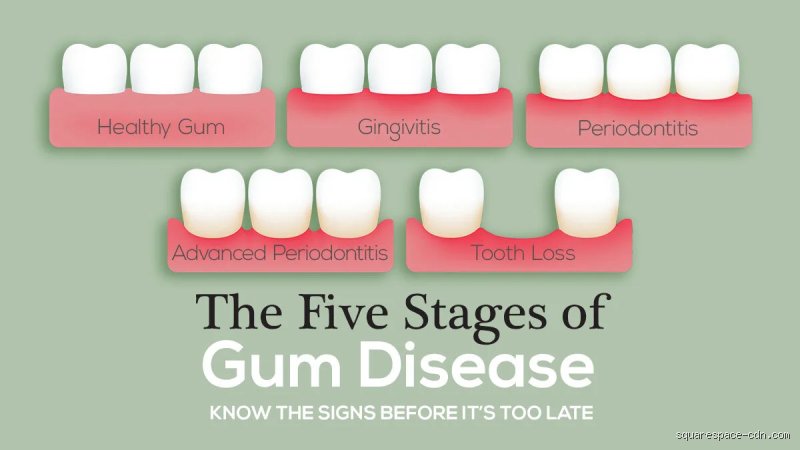
Your mouth is a complex ecosystem where billions of microbes constantly battle for territory. When plaque—a sticky film of bacteria—accumulates along the gingival margin, the body launches an immune response. This initial stage is gingivitis. Except that it is entirely superficial. The architecture of the periodontium, which includes the gingiva, the periodontal ligament, and the alveolar bone, remains fully intact despite the redness and swelling.
Gingivitis vs. Periodontitis: Where the Damage Becomes Permanent
Here is where it gets tricky. Gingivitis is a reversible inflammatory lesion, meaning that if a dental hygienist scrapes away the calcified tartar (calculus) and you step up your flossing game, your tissues return to baseline. No permanent harm done. But if left unchecked, the chronic inflammation triggers an osteoclastic response. This means your own immune system, in a misguided attempt to retreat from the invading bacteria, begins to dissolve the very bone supporting your teeth. Once that alveolar bone liquefies, the damage is done; you cannot naturally regrow that lost foundation, and that changes everything.
The Role of the Sulcus and the 4mm Flashpoint
Dentists measure this destruction using a periodontal probe, dropping a tiny millimeter ruler into the space between your tooth and gum. A healthy sulcus measures between 1 and 3 millimeters. When bacteria destroy the attachment fibers, this space deepens into a periodontal pocket. A reading of 4 millimeters or higher indicates that the attachment loss has begun. I have seen patients shocked to discover that a completely painless 6mm pocket means they have already lost a significant portion of the bone holding their molars in place. Pain, unfortunately, is a terrible metric for severity in the oral cavity.
The Cellular Turning Point: What Actually Happens When It is Too Late?
To truly understand why you cannot reverse gum disease past a certain marker, we have to look at the microscopic battlefield. The primary drivers of this destruction are not actually the bacteria themselves, but rather your body's enzymatic response to them. Matrix metalloproteinases (MMPs), specifically MMP-8, flood the tissue to break down old collagen during the fight, but in a chronic state, they run amok and destroy the healthy extracellular matrix of your gums.
The Irreversible Destruction of the Alveolar Bone
Think of your tooth as a skyscraper and the alveolar bone as the bedrock it anchors into. In a landmark 2018 study published in the Journal of Clinical Periodontology, researchers demonstrated that once host-derived inflammatory mediators like Interleukin-1 beta (IL-1β) and Tumor Necrosis Factor-alpha (TNF-α) reach a threshold concentration in the gingival crevicular fluid, bone resorption accelerates exponentially. Because bone remodeling in the jaw requires a highly specific scaffold, horizontal bone loss—where the entire height of the bone drops uniformly—cannot be coaxed into growing back upward through standard hygiene means. The bone is gone, vanished into the systemic circulation, leaving the tooth root exposed and vulnerable.
The Disruption of the Periodontal Ligament (PDL)
And then there is the periodontal ligament, a stunningly complex network of collagen fibers that acts as a shock absorber for your teeth during mastication. Each tooth is suspended in its socket by these microscopic bungee cords. When periodontitis takes hold, the chronic bacterial onslaught severs these connections permanently. Without the PDL transmitting mechanical forces to the bone, the body assumes the bone is no longer needed, which explains why the degradation becomes a self-fulfilling prophecy. Once the ligament is necrotic, the tooth begins to wobble, a terrifying symptom that usually drives patients to the clinic far too late.
Clinical Realities: Diagnosing the Point of No Return
So, how do we determine if you have crossed into the zone of no return? It is not a guessing game; it requires a combination of clinical probing depths, radiographic imaging, and an assessment of tooth mobility. Clinicians use the staging and grading system updated by the American Academy of Periodontology (AAP) in 2017 to categorize the wreckage.
Stage III and Stage IV Periodontitis
If you are diagnosed with Stage I or II periodontitis, you are dealing with mild to moderate bone loss, usually manageable with aggressive therapy. But Stage III and Stage IV represent the true "too late for reversal" territory. At this juncture, you are looking at probing depths greater than or equal to 6mm, vertical bone loss, and furcation involvements—where the bone between the roots of a multi-rooted tooth has melted away entirely. People don't think about this enough, but when a dentist can pass a metal instrument entirely through the space underneath your molar where bone used to be, your oral health strategy must pivot entirely from prevention to damage control.
Radiographic Evidence of Tooth Mobility
X-rays do not lie. A panoramic or periapical radiograph reveals the definitive level of the interdental bone crest. In a healthy mouth, the bone sits about 1 to 2mm below the point where the enamel ends and the root begins. In advanced periodontitis, the bone line drops halfway down the root, or worse, hovers near the apex. When radiographs show more than 50% bone loss, tooth mobility becomes inevitable. Teeth start drifting apart, creating unsightly gaps where none existed before, which makes eating an exercise in discomfort. At this stage, we are far from it being a matter of just flossing better.
Therapeutic Shifts: Reversal vs. Management and Stability
When we say you cannot reverse gum disease, we mean you cannot restore the original anatomy. Yet, the distinction between "curing" and "stabilizing" is where many patients get confused. Experts disagree on whether certain advanced cases can ever be deemed truly stable, but the consensus remains that we can halt the progression of the disease even if we cannot rebuild the past.
Scaling and Root Planing (SRP) vs. Periodontal Maintenance
For gingivitis, a simple prophylaxis suffices. For periodontitis, the baseline intervention is scaling and root planing, a deep cleaning done under local anesthesia where the clinician scrapes deep beneath the gumline to smooth the root surfaces and remove embedded bacterial toxins. But here is the catch: after an SRP, you are never a regular cleaning patient again. You transition to periodontal maintenance every three months. Why? Because the pathogenic bacteria, specifically Porphyromonas gingivalis, repopulate the deep pockets within 90 to 120 days. Skipping these maintenance appointments means the inflammatory cascade restarts immediately, rendering the initial treatment useless.
The Role of Regenerative Surgical Interventions
Can modern science cheat the system? Sometimes, yes, but it is highly situational. Guided tissue regeneration (GTR) using bone grafts and membranes can occasionally repair deep, narrow vertical bone defects caused by localized trauma or specific infection patterns. However, if you have generalized horizontal bone loss across your entire jaw from decades of neglect, a bone graft cannot simply be smeared across the arch like spackle on a drywall. The tissue architecture will not support it, meaning that for the vast majority of advanced sufferers, the goal is merely keeping the remaining teeth in the mouth for as long as possible.
Common myths clouding your periodontal prognosis
People love Google. They browse forums, read horror stories, and convince themselves that a little pink in the sink means impending edentulism. Let's be clear: bleeding gums are never normal, yet they do not signify immediate tooth loss. The problem is that patients frequently oscillate between total panic and absolute denial.
The brush-it-away fallacy
You cannot scrub away a structural deficit. When bacteria infiltrate below the gingival margin, your standard manual toothbrush becomes effectively useless. Aggressive scrubbing actually worsens the situation by tearing the fragile, inflamed attachment apparatus. Patients assume harder brushing cleans deeper, which explains why we see so many cases of severe root exposure combined with active infection. Statistics show that over forty percent of adults over thirty display signs of periodontitis, yet a massive portion of them believe switching toothpaste brands will miraculously regrow their jawbone.
The pain barometer mistake
Is it too late to reverse gum disease if nothing hurts? Absolutely not. Chronic periodontitis is notoriously silent. It acts like hypertension of the mouth. The bone dissolves quietly while you go about your day. By the time a molar becomes loose or starts throbbing, you are no longer dealing with a reversible condition; you are staring down the barrel of surgical splinting or extractions. Waiting for physical agony before booking a specialist appointment is a fast track to the prosthodontist's chair.
The silent threat of the systemic tax
We need to talk about what happens when your body fights a war that never ends. Periodontitis is not merely an isolated oral issue; it is a vascular gateway. Your gums are highly vascularized tissues. When they remain ulcerated for years, billions of anaerobic bacteria slip directly into your bloodstream daily.
The macrophage overload
Your immune system gets exhausted. Constant systemic inflammation strains your liver, which pumps out C-reactive protein in response to the oral chaos. Except that nobody looks at their mouth when diagnosing systemic fatigue or cardiovascular strain. Research correlates severe attachment loss with a twenty-four percent increase in the risk of developing premature coronary artery disease. Your body is paying a continuous metabolic tax to keep the oral infection contained, which saps your overall vitality. When is it too late to reverse gum disease systemically? The moment those inflammatory cascades trigger secondary cellular damage across your body, reversing the oral damage won't instantly undo the systemic wear and tear.
Frequently Asked Questions
Can bone lost from advanced periodontitis ever grow back naturally?
No, alveolar bone does not spontaneously regenerate once the architectural scaffolding has vanished. While early gingivitis allows for total tissue recovery, true periodontitis causes irreversible destruction of the alveolar socket. Modern regenerative dentistry can utilize specialized bone grafts, enamel matrix derivatives, or guided tissue membranes to trick the body into rebuilding up to sixty percent of lost support in specific, vertical defects. Horizontal bone loss, however, remains notoriously stubborn to fix. Therefore, while you can halt the progression of the disease and solidify the remaining structures, you will never naturally regain the youthful bone height you possessed in your twenties.
How long does it take to stabilize shifting teeth?
Stabilization depends heavily on your compliance and the specific degree of mobility present. Expect a minimum of three to six months of intensive periodontal therapy, including deep root planing and potentially antibiotic chips, before fibers begin to tighten. If the tooth exhibits Class Three mobility (moving more than two millimeters in any direction), mechanical splinting or extraction becomes inevitable. Clinical data suggests that successful deep scaling can reduce pocket depths by an average of one to two millimeters across the mouth, allowing the surrounding gingiva to clamp tightly around the root. But if you keep smoking or skip your three-month maintenance recare visits, those teeth will start dancing again almost immediately.
Will insurance cover the cost of laser periodontal therapy?
Insurance companies are notoriously conservative, often viewing advanced laser procedures as experimental luxuries rather than clinical necessities. Most standard policies will reimburse you for traditional scaling and root planing under specific codes, but they frequently leave the patient covering the balance for advanced laser disinfection. This financial hurdle causes many individuals to delay necessary interventions, prompting them to ask when is it too late to reverse gum disease only after their teeth become unsalvageable. Out-of-pocket costs for full-mouth laser protocols can range from two thousand to over eight thousand dollars depending on severity. (Yes, saving your natural dentition is expensive, but it remains vastly cheaper than dental implants.)
A definitive verdict on your dental destiny
Stop waiting for a miracle rinse or a magical supplement to fix a structural, bacterial meltdown. The line between a manageable chronic condition and irreversible dental disability is thinner than you think. We know our clinical limitations; we cannot resurrect dead tissue. If you ignore the bleeding today, you are actively choosing a future of removable partial dentures and compromised nutrition. Take a stand before the microscopic pathogens dictate your systemic health. Go get your pocket depths measured by a professional who owns a periodontal probe, not a search engine. Your smile, your cardiovascular system, and your jawbone will thank you for the sudden dose of reality.