Survival is only the first hurdle. When a surgeon clips or coils a bulge in the cerebral wall, they are essentially performing high-stakes plumbing on the most delicate biological computer in existence. You walk out of the hospital feeling like a survivor, but the reality is that your vascular system is currently held together by a mix of titanium and hope. People don't think about this enough, but the weeks following a craniotomy or endovascular procedure are arguably more dangerous than the surgery itself because the "patient" suddenly feels capable of doing things they absolutely should not. I have seen patients try to mow the lawn six days after a discharge because they felt fine, only to end up back in the ER with a localized hemorrhage. That changes everything. The brain doesn't just bounce back; it recalibrates with agonizing slowness.
The Biological Reality of a Repaired Vessel Wall
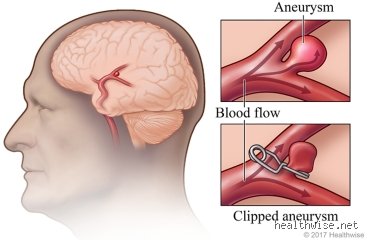
Understanding the Structural Vulnerability of the Circle of Willis
Most aneurysms occur at the bifurcations of the Circle of Willis, a ring-like arterial structure at the base of the brain that ensures blood flow even if one "pipe" gets clogged. When a neurosurgeon places a micro-vascular clip across the neck of an aneurysm, they are mechanicaly excluding that weak spot from the high-pressure circulation. However, the surrounding endothelial tissue is traumatized. Because the blood vessel has been stretched and potentially thinned by the saccular dilation, the immediate post-operative period is characterized by significant inflammation. The issue remains that while the clip is permanent, the vessel's ability to withstand a sudden systolic blood pressure surge over 160 mmHg is severely compromised during the first month. You aren't just healing a wound on your scalp; you are waiting for a microscopic scarring process to cement the repair in place.
Why the Type of Procedure Dictates Your Limitations
Is there a difference between "open" and "closed" restrictions? Honestly, experts disagree on the exact timeline, but the physiological demands vary wildly. If you underwent a craniotomy (the "open" method), your brain has literally been handled, and your skull has been breached. The dura mater needs time to seal. Conversely, endovascular coiling or the placement of a Pipeline embolization device involves threading a catheter from the femoral artery in the groin up to the brain. While the "brain" part feels less invasive, the risk of thromboembolic events remains high. You might not have a massive scar on your head, but the internal "plumbing" is just as fragile. And that is where it gets tricky—the lack of an external wound often lures patients into a false sense of security that leads to overexertion.
Physical Restrictions: Where It Gets Tricky for Active Patients
The Danger of the Valsalva Maneuver and Intracranial Pressure
The most immediate "no-go" is anything that causes you to strain. This is formally known as the Valsalva maneuver. Think about the last time you tried to open a stuck pickle jar or lifted a heavy box of books. You naturally hold your breath and bear down. In that split second, your intrathoracic pressure skyrockets, which in turn causes a sharp spike in the pressure within your skull. For a cerebral aneurysm repair that is only ten days old, this is like putting 100 pounds of air into a tire rated for 30. As a result: you must avoid lifting anything heavier than a gallon of milk (roughly 8 pounds or 3.6 kilograms) for at least six weeks. But it isn't just weights. Even straining on the toilet can be hazardous, which is why surgeons almost universally prescribe stool softeners as a mandatory part of the post-op cocktail. We're far from the days of total bed rest, yet the "no strain" rule is absolute.
Reevaluating Exercise and the Myth of "Getting Back to Normal"
But what about walking or light activity? While light walking is encouraged to prevent Deep Vein Thrombosis (DVT), you cannot engage in any activity that raises your heart rate significantly. No jogging, no swimming, and definitely no hot yoga. Heat causes vasodilation, and when your vessels dilate, the pressure dynamics around the aneurysm clip or coil mass shift. Most neurosurgical protocols from institutions like the Mayo Clinic suggest waiting a minimum of 4 to 12 weeks before resuming "moderate" cardio. The thing is, your brain's autoregulation—the system that keeps blood flow steady despite changes in your body—is often "stunned" after a subarachnoid hemorrhage or even a preventive surgery. If you push it too fast, you risk vasospasm, where the arteries narrow down and starve the brain of oxygen, potentially leading to a delayed stroke.
Cognitive and Environmental No-Fly Zones
The Heavy Burden of Sensory Overload
You cannot ignore the "brain drain" that follows neurosurgery. Most people focus on the physical, yet the cognitive restrictions are just as vital. For the first two weeks, you should not spend hours staring at blue-light-emitting screens or engaging in complex, high-stress decision-making. Why? Because cerebral metabolic demand increases when you are stressed or over-stimulated. A healing brain has limited resources; if you use all your "fuel" trying to finish a work spreadsheet, there is less energy available for cellular repair and the management of post-operative edema (swelling). This explains why many patients experience "crashes"—sudden, overwhelming fatigue—after simply having a long conversation with a visitor. It is not just "being tired"—it is your brain signaling that its interstitial fluid management is overwhelmed.
Travel Restrictions and the Altitudinal Risk
Can you fly after an aneurysm surgery? Generally, the answer is a hard "no" for the first 4 to 6 weeks. While modern cabins are pressurized, they are usually pressurized to an equivalent of 6,000 to 8,000 feet. This slight decrease in partial pressure of oxygen and changes in atmospheric pressure can cause trapped air (pneumocephalus)—often present after a craniotomy—to expand. Even in endovascular cases, the risk of a blood clot during a long-haul flight is significantly elevated because your blood's coagulation profile is altered following the introduction of foreign materials like platinum coils or flow diverters. Most surgeons will require a follow-up CT Angiogram (CTA) or MRA to confirm the repair is stable before they let you step foot on a Boeing 737.
Comparing Clipping vs. Coiling Recovery Mandates
The Disparity in Immediate Post-Op Restrictions
When comparing microsurgical clipping to endovascular coiling, the immediate "don'ts" actually differ in their focus. With clipping, the primary concern is often the incisional integrity and the risk of cerebrospinal fluid (CSF) leaks; therefore, you cannot submerge your head in water (no baths or pools) for several weeks to prevent infection. In coiling, the entry point is the femoral artery. Consequently, for the first week, you cannot take stairs aggressively or sit in a cramped position that might "kink" the access site, as this could cause a pseudoaneurysm or a massive hematoma in the leg. Which explains why coiling patients often feel "fine" in their heads but are restricted by their groins. It is a strange irony: the brain repair is hidden, but the leg wound dictates the first 48 hours of movement.
Long-Term Monitoring: The "Never-Ending" Restriction
There is a lingering misconception that once the surgery is done, the "restrictions" disappear after the six-month check-up. But the reality is that once you've had one aneurysm, your vasculature has proven it is prone to weakening of the tunica media. This means you can never truly return to certain habits. Smoking is the big one. If you have had an aneurysm surgery, you can never smoke again. Nicotine is a potent vasoconstrictor that also degrades the collagen in your vessel walls. Data shows that smokers have a significantly higher rate of aneurysm recurrence or the formation of "de novo" aneurysms elsewhere in the brain. It is a non-negotiable lifetime ban. Same goes for unmanaged hypertension; if you stop taking your blood pressure meds because you "feel cured," you are essentially inviting the pressure to find the next weakest link in your arterial chain.
Common mistakes and misconceptions
The fallacy of the invisible wound
You woke up, the anesthesia fog lifted, and because there is no massive scar across your scalp, you assume the interior plumbing is fixed for good. This is a dangerous trap. Patients often believe that endovascular coiling or stenting requires less downtime than a traditional craniotomy. The issue remains that while your skin looks pristine, your cerebrovascular architecture is undergoing a violent remodeling process. One common error is returning to high-intensity interval training within the first month. Because your heart rate spikes, the internal pressure against that newly placed clip or coil set could jeopardize the healing endothelium. Let us be clear: your brain does not care how small the incision was when your blood pressure hits 180 mmHg during a heavy squat.
The dehydration trap
Why do so many survivors end up back in the ER with preventable headaches? They forget to drink water. People think coffee is fine, but caffeine is a vasoconstrictor that can mimic the sensation of a looming complication. The problem is that post-surgical patients often fear frequent bathroom trips more than they fear a minor ischemic event caused by thickened, sluggish blood. Research indicates that maintaining a steady MAP (Mean Arterial Pressure) is significantly easier when systemic volume is consistent. If you are not hitting at least 2.5 liters of fluid daily, you are playing a risky game with your cognitive recovery speed. Do you really want to stall your progress because you were too lazy to carry a water bottle?
The hidden cognitive fatigue threshold
The sensory overload tax
Neurologists often fail to mention that your brain’s "filter" is temporarily broken. You might think you can handle a trip to a crowded shopping mall or a loud family dinner three weeks post-op, yet the reality is usually a crushing migraine or a sudden emotional meltdown. This phenomenon, often called neuro-fatigue, is not a lack of willpower. It is a biological bottleneck. Your neural pathways are rerouting signals around the surgical site, which consumes an immense amount of metabolic glucose. But trying to "power through" this exhaustion actually delays long-term neuroplasticity. As a result: you must treat your mental energy like a finite bank account. If you spend it all on a two-hour Zoom call, you will be bankrupt for the next forty-eight hours. It is an annoying reality, (even if your boss disagrees), but your gray matter requires a boring, low-stimulation environment to truly knit itself back together.
Frequently Asked Questions
When can I safely fly on a commercial airplane again?
The standard medical consensus usually suggests waiting at least four to six weeks, though some neurosurgeons demand a full three-month window before boarding a pressurized cabin. The primary concern is not just the altitude, but the hypoxic environment of the aircraft which can cause slight cerebral edema in sensitive tissues. Statistics show that cabin pressure typically mimics an altitude of 6,000 to 8,000 feet, potentially reducing oxygen saturation in your blood by 3% to 5%. For a healthy brain, this is negligible, but for a vessel recovering from a subarachnoid hemorrhage, it is a significant stressor. You must obtain a formal clearance from your specialist because a mid-air complication is a logistical nightmare no one wants to navigate.
Is it safe to resume sexual activity shortly after discharge?
While this is a sensitive topic, it is one of the most frequent questions patients are too embarrassed to ask. Most clinical guidelines permit light intimacy once you can climb two flights of stairs without shortness of breath or a pounding headache. However, the sudden catecholamine surge during orgasm can cause a transient but sharp spike in systolic blood pressure. Data suggests these spikes can briefly exceed 200 mmHg in some individuals, which is exactly what you cannot do after an aneurysm surgery during the first fourteen days. Stick to a conservative timeline and keep the intensity low until your first follow-up MRA or CT angiogram confirms the repair is stable. Which explains why "taking it slow" is not just romantic advice, but a literal medical requirement for your safety.
Can I drink alcohol or use nicotine during the recovery phase?
Nicotine is the absolute enemy of a successful recovery because it is a potent vasoconstrictor that significantly increases the risk of vasospasm and delayed cerebral ischemia. Studies show that smokers have a 300% higher rate of aneurysm recurrence compared to non-smokers, making cessation the single most important lifestyle change you can implement. Alcohol is slightly different but equally problematic as it thins the blood and interferes with the seizure prophylaxis medications often prescribed post-surgery. Even a single glass of wine can disrupt your REM cycle, preventing the deep sleep necessary for glymphatic clearance of surgical debris. In short: if you want your brain to heal, you have to stop poisoning it with substances that fluctuate your vascular tone.
Engaged Synthesis
Recovery is not a linear climb; it is a frustrating series of tactical retreats. We live in a culture that fetishizes "grinding" and "bouncing back," but your cerebral arteries do not subscribe to your productivity goals. The hardest part of this journey is acknowledging that physical stillness is the most productive action you can take. I take the firm stance that patients are discharged far too early with far too little education on the sheer fragility of their neurovascular state. You are not a broken machine that has been soldered back together; you are a living ecosystem that has survived a catastrophic tectonic shift. Respect the timeline, or the timeline will eventually force you to respect it through a relapse. Your only job right now is to be a quiet observer of your own healing, refusing to rush a process that has no shortcut.