The Pancreatic Tinderbox: Why Graded Diagnosis Shifts So Fast
The pancreas is a volatile little organ tucked behind the stomach, responsible for secreting digestive enzymes that normally activate only when they reach the duodenum. When something disrupts this delicate pipeline—usually a gallstone getting stuck in the common bile duct or metabolic stress from heavy alcohol consumption—those potent enzymes activate prematurely right inside the pancreas itself. It essentially starts digesting itself, a process we call autodigestion. People don't think about this enough, but a mild bout can morph into a necrotic nightmare with terrifying speed. Because the organ sits so close to major vascular structures and the celiac plexus, the resulting inflammation doesn't stay localized for long.
The Atlanta Classification Benchmark
Clinicians rely heavily on the Revised Atlanta Classification to draw a line in the sand between different stages of this disease. Mild acute pancreatitis features no organ failure and no local complications, usually clearing up with some aggressive intravenous fluids and bowel rest. Then there is the moderate tier, where transient organ failure resolves within 48 hours, perhaps accompanied by a fluid collection. But severe acute pancreatitis? That is defined by persistent organ failure lasting beyond that 48-hour window, which changes everything for the patient's prognosis. I have seen cases start with minor nausea on a Tuesday and escalate to complete respiratory collapse by Thursday night.
The Real Danger of Pancreatic Necrosis
When the inflammation gets severe enough, it cuts off the blood supply to portions of the tissue. This dead tissue, or necrosis, is a sterile breeding ground for trouble, but the issue remains that if bacteria from the gut translocate into this dead zone, you are looking at infected necrosis. Where it gets tricky is differentiating sterile necrosis from infected fluid collections without doing a risky needle biopsy. If infection sets in, mortality rates double, forcing teams into a corner where they must use high-tier antibiotics or resort to minimally invasive drainage procedures.
Early Warning Signs: How to Tell the Severity of Pancreatitis at the Bedside
You cannot determine severity simply by how loudly a patient is screaming in the emergency room. Pain intensity in the epigastric region, while notoriously excruciating and radiating straight through to the back, correlates poorly with the actual degree of tissue destruction. Instead, we have to look at systemic vitals. Is the patient tachycardic with a heart rate clearing 110 beats per minute? Are they tachypneic, breathing more than 24 times a minute? These are the early footprints of systemic inflammatory response syndrome, or SIRS, which acts as our loudest alarm bell in the first few hours of admission.
The Hidden Signals in Your Vitals
A plummeting blood pressure that refuses to budge despite running two liters of normal saline through a wide-bore IV is a catastrophic sign. This indicates third-spacing, a phenomenon where fluid leaks out of the capillaries into the interstitial spaces of the abdomen, leaving the vascular system bone-dry. Why does this happen? The sheer volume of cytokines released during the initial autophagic meltdown destroys endothelial integrity. If the patient shows altered mental status or confusion, the brain isn't getting perfused properly, and we are already losing the battle against shock.
The Physical Exam Flags
On rare occasions, the physical exam itself yields unmistakable clues of retroperitoneal hemorrhage. You might notice a faint, bluish bruising around the umbilicus, famously known as Cullen's sign, or along the flanks, which we call Grey Turner's sign. Honestly, it's unclear why these classic signs appear in fewer than 3% of severe cases, but when they do show up, usually days into the illness, they signify massive hemorrhagic pancreatitis. It is an ominous clinical finding that usually means the patient needs an immediate ticket to an intensive care unit bed.
The Lab Analytics: Deciphering the Biochemical Storm
Every rookie clinician wants to check amylase and lipase levels immediately to gauge how bad things are, yet this is a massive trap because the absolute numbers do not correlate with severity at all. A lipase level that is ten times the upper limit of normal can occur in a mild case that resolves in 48 hours, while a severely necrotic pancreas might produce barely elevated enzymes because the tissue is too dead to secrete anything. We must look elsewhere on the metabolic panel to get a real glimpse into the future.
Hematocrit and Blood Urea Nitrogen Dynamics
The true crystal ball lies in tracking hematocrit and blood urea nitrogen, commonly known as BUN. A high baseline hematocrit above 44% upon admission, or a value that fails to decrease within 24 hours of fluid resuscitation, tells us the blood is dangerously concentrated due to massive fluid loss. Even more telling is a rising BUN level; an increase of more than 5 milligrams per deciliter within the first 24 hours of hospitalization is a premier predictor of mortality. It reflects both severe intravascular dehydration and early acute kidney injury, two components that can rapidly accelerate multi-organ failure.
Inflammatory Biomarkers and Calcium Drops
Another metric we watch closely is C-reactive protein, or CRP. If the CRP level crosses 150 milligrams per liter at the 48-hour mark, it serves as a reliable lagging indicator of pancreatic necrosis. Then there is serum calcium to consider. When fat necrosis occurs around the pancreas, it releases free fatty acids that bind to calcium ions, a process called saponification that literally turns fat into soap. As a result, serum calcium drops below 8 milligrams per deciliter, stripping the body of a critical electrolyte needed for cardiac stability and signaling a highly destructive local process.
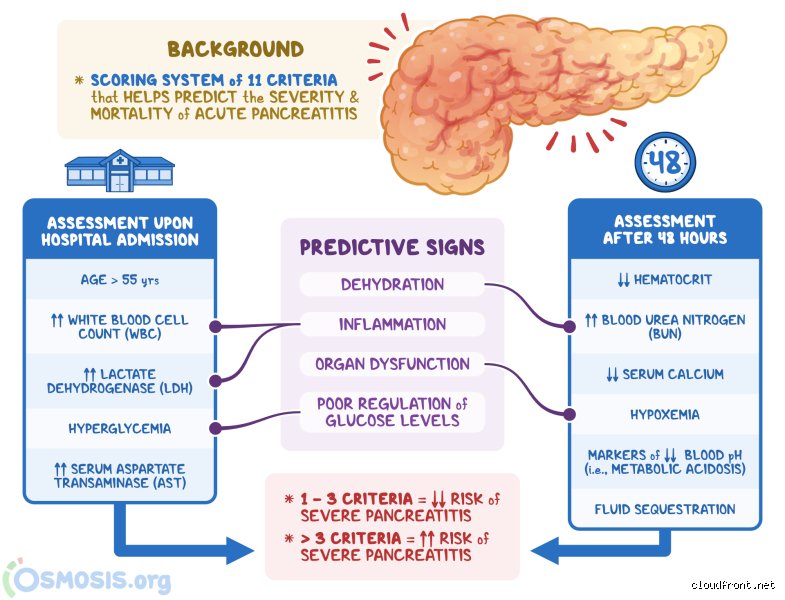
Predictive Scoring Systems vs. Clinical Instinct
To standardize how we tell the severity of pancreatitis, medicine has cooked up several complex scoring matrices over the decades. The oldest and most famous is the Ranson Criteria, developed back in 1974, which requires evaluating five parameters at admission—like an age over 55 and a white blood cell count over 16,000—and then checking another six parameters at the 48-hour mark. This 48-hour delay is the system's Achilles' heel because you cannot afford to wait two whole days just to decide if a patient needs an ICU bed. Experts disagree on whether we should abandon Ranson entirely, but in a fast-paced emergency department, it is often too slow to be useful.
The Modern Speed of BISAP
Enter the BISAP score, a much slicker, five-point tool that can be calculated within the first 24 hours of triage. It tracks blood urea nitrogen over 25, impaired mental status, the presence of SIRS, an age over 60, and the detection of a pleural effusion on a chest X-ray. If a patient scores a 3 or higher on the BISAP scale, their risk of mortality jumps exponentially, which explains why many modern triage protocols have swapped Ranson out for this faster alternative. It allows us to catch the downward spiral before the patient completely decompensates.
APACHE II: The Heavy Artillery
For patients who are already in the ICU, we roll out the APACHE II scoring system, which is a beast of a matrix utilizing 12 different physiological variables ranging from arterial pH to temperature and neurological status. It is incredibly accurate and can be calculated daily to track whether the patient is improving or getting worse, but it requires a mountain of data points. A score of 8 or higher on the APACHE II scale usually means you are dealing with severe acute pancreatitis, demanding aggressive intervention and continuous monitoring of vital organ systems.