The Messy Reality of Identifying Skin Damage Beyond the Surface
We tend to think of skin as a simple wrapper, but when high-heat energy hits the dermis, the biological response is anything but predictable. The thing is, what looks like a simple "ouch" moment over a boiling pot of pasta can evolve into a deep-tissue nightmare within hours because heat continues to radiate inward even after you pull your hand away. Most people assume pain is the primary indicator of severity, yet the paradox of the human nervous system dictates that the most life-threatening burns are often the ones that don't hurt at all. Because the nerve endings have been incinerated—literally turned to carbon—your brain receives no signal of the catastrophe occurring beneath the surface. I have seen patients walk into clinics calmly with third-degree charring simply because their pain receptors were offline, which is a terrifyingly deceptive scenario for the untrained eye.
The Anatomy of Thermal Trauma
Every burn is a transfer of energy that disrupts the cellular structure of the integumentary system. While textbooks love to categorize these into neat boxes, the issue remains that a single injury site often presents a mosaic of different depths. You might have a central core of dead tissue surrounded by a ring of blistering, which is then bordered by a wide margin of simple redness. This "zone of stasis" is where the battle for your skin is won or lost. If you don't cool the area correctly—and no, butter or ice is not the answer—the damage spreads like a slow-motion ripple in a pond. Experts disagree on exactly how long the cooling process should last, but the current consensus leans toward twenty minutes of cool, running water. Is it frustrating to stand over a sink for a third of an hour? Absolutely, but it is the only way to arrest the thermal progression before it migrates from a minor nuisance to a surgical necessity.
Decoding the Three-Tiered System of Burn Severity
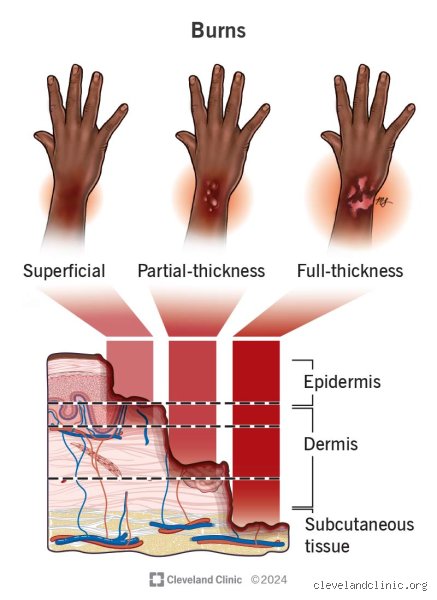
Medical professionals rely on a classification system that has shifted away from the old-fashioned "degrees" toward a more descriptive terminology involving thickness. First-degree burns, or superficial burns, only affect the epidermis. Think of the classic 2024 Coachella sunburn where your skin feels tight and hot but remains intact. These are rarely serious unless they cover the entire body. But where it gets tricky is the transition into the second tier, known as partial-thickness burns. These involve the dermis, the layer containing your sweat glands and hair follicles. If you see clear fluid leaking from a raised bubble, you have officially crossed the line into a territory that requires vigilant monitoring. These blisters act as a natural, sterile bandage, and popping them is perhaps the most common—and dangerous—mistake a person can make at home.
When Blisters Signal a Deeper Crisis
When we talk about partial-thickness injuries, we have to distinguish between superficial and deep. A superficial partial-thickness burn will blanch—turn white—when you press it and then quickly turn red again. This indicates that the capillary refill is still functional. However, if the area is a mottled red and white and does not change color when pressed, the blood vessels are likely compromised. This isn't just a minor cosmetic issue; it is a sign that the skin may not be able to heal itself without intervention. In the United States alone, approximately 486,000 people receive medical treatment for burns annually, and a significant portion of those are these "tweener" burns that people tried to treat with home remedies for three days before the smell of infection set in. Honestly, it's unclear why the general public still clings to the idea that a blister is just a "big pimple," but that misconception keeps burn units very busy.
The Silent Danger of Full-Thickness Destruction
Full-thickness burns, formerly called third-degree, are the undisputed heavyweights of trauma. These penetrate through every layer of the skin and often reach the subcutaneous fat or muscle. The texture is the giveaway here. Instead of the wet, weeping look of a lesser injury, a serious burn feels like dry parchment or stiff leather. It may look white, brown, or even black. Because the skin has lost its elasticity, it can actually act as a tourniquet. In cases where these burns encircle a limb—what doctors call a circumferential burn—the swelling can cut off blood flow entirely. This leads to a procedure called an escharotomy, where a surgeon must slice through the dead skin to allow the limb to breathe. People don't think about this enough when they are messing around with backyard fire pits or industrial chemicals.
Technical Indicators of a Medical Emergency
Size matters just as much as depth when determining how to tell if a burn is minor or serious. A common rule of thumb in emergency medicine is the "Rule of Nines," which divides the body into sections representing 9 percent of the total surface area. For a quick assessment at home, you can use the "palmar surface" method: the patient's palm, including the fingers, represents roughly 1 percent of their body surface area. If the burned area is larger than three palms, you are far from a minor injury. This is especially true for children and the elderly, whose skin is thinner and whose physiological reserves are much lower. A 10 percent burn on a healthy 25-year-old is a bad day; a 10 percent burn on a 3-year-old is a life-threatening crisis that can lead to rapid dehydration and shock.
Critical Zones and Functional Impairment
Location is the silent tie-breaker in the "minor vs. serious" debate. A small, deep burn on your thigh might be manageable at a local urgent care, but that same burn on your eyelid, lip, or genital area is an automatic ticket to a specialized burn center. Why? Because the scarring in these areas causes functional catastrophe. If the skin on your knuckle heals too tightly, you may never be able to make a fist again. This is why any burn that crosses a joint is considered serious by default. Furthermore, any burn involving the face or neck carries the risk of inhalation injury. If there are singed nasal hairs or soot in the saliva, the heat has likely scorched the airway. The throat can swell shut in minutes, a process that is as relentless as it is terrifying, making the external skin damage the least of the patient's worries.
Comparing Thermal, Chemical, and Electrical Insults
Not all burns are created by fire or steam, and the source of the injury drastically changes the diagnostic criteria. Chemical burns are particularly insidious because they continue to eat through tissue until the agent is completely neutralized. An acid burn might look like a simple red patch initially, yet it can continue to drill downward for hours. Alkaline burns, caused by substances like drain cleaner or wet cement, are even worse because they liquefy the fat in your skin through a process called saponification. It's essentially like your body is being turned into soap from the inside out. You cannot judge these by the same visual standards as a sunburn; any chemical exposure that causes skin discoloration or pain should be treated as a serious event.
The Invisible Path of Electrical Damage
Electrical burns are the ultimate "iceberg" injuries. What you see on the surface—usually a small, charred "entrance" wound and an "exit" wound elsewhere—is almost never the full story. The electricity travels through the body's internal tissues, which offer the least resistance, namely nerves and blood vessels. This generates massive internal heat that can cook muscles and organs while the skin looks relatively unscathed. As a result, cardiac arrhythmias and kidney failure are more common in electrical burn victims than skin infections. If you have been shocked by a high-voltage source, the appearance of the skin is irrelevant; the potential for your heart to stop two hours later makes it a serious medical emergency by definition. Yet, people often shrug these off if they don't see a "big enough" wound, which is a gamble I would never recommend taking.
Dangerous Myths and the Butter Trap
Kitchen lore is a graveyard of terrible medical advice that effectively turns a manageable injury into a deep-tissue catastrophe. Let's be clear: applying butter or margarine to a fresh heat injury is an invitation for bacterial colonization. The fat traps the thermal energy. It continues to cook your dermis long after you have moved away from the stove. The problem is that people mistake the initial cooling sensation of cold fat for actual healing, yet they are merely insulating a metabolic fire. Stop doing it. Because household condiments are non-sterile, you are essentially introducing pathogens into a site where the primary immune barrier has already vanished.
The Ice Water Fallacy
You might think plunging a charred hand into a bucket of ice is the apex of first aid. It is not. Extreme cold causes rapid vasoconstriction, which chokes off the blood supply to the already struggling tissue. As a result: you risk converting a partial-thickness injury into full-thickness necrosis simply by over-chilling. Aim for cool, running tap water for exactly twenty minutes. It sounds tedious. It is. But that specific timeframe is backed by clinical data showing a significant reduction in the need for future skin grafting. Ice is for drinks, not for raw nerves.
Adhesive Bandages and the Peeling Nightmare
Generic plastic bandages are the enemy of a weeping blister. If you stick a standard adhesive strip directly onto a de-roofed burn, you will inevitably rip off the regenerating epithelium during the next dressing change. Use non-adherent silicone or petroleum-based gauze. Except that most people do not keep these in their cabinets, leading to a frantic Sunday night trip to the pharmacy. If it sticks, it kills the new skin cells trying to bridge the gap.
The Silent Progression of Chemical Leaching
Most experts focus on heat, but the most deceptive way to tell if a burn is minor or serious involves pH levels. A chemical burn often looks underwhelming at the five-minute mark. Unlike thermal damage, which hits its peak almost instantly, alkaline substances like lye or drain cleaner saponify the fats in your skin. They melt you from the inside out. You might feel a slight tingle while a deep liquefaction necrosis is liquefying your subcutaneous layers. (This is exactly as gross as it sounds). Always check the Material Safety Data Sheet if you can, because water alone sometimes triggers an exothermic reaction with certain powders, making the situation worse.
The 24-Hour Re-Evaluation Rule
Burn depth is a dynamic process rather than a static snapshot. An injury that appears to be a simple "minor" first-degree redness at noon can evolve into a blistering second-degree mess by the following morning. This is known as burn wound conversion. We often overestimate our ability to self-diagnose in the heat of the moment. If the pain intensity spikes after the first six hours, or if a murky fluid begins to leak, your initial "minor" label was wrong. Expert triage requires a follow-up look once the initial inflammatory surge has stabilized.
Frequently Asked Questions
When does the total body surface area dictate a hospital visit?
The "Rule of Nines" is the gold standard used by paramedics to calculate the severity of the trauma. If a partial-thickness injury covers more than 10 percent of a child's body or 15 percent of an adult's, the risk of systemic hypovolemic shock becomes a statistical certainty. You can use your own palm to represent roughly 1 percent of your body area. Any cluster of blisters larger than ten of your palms requires immediate intravenous fluid resuscitation in a clinical setting. The issue remains that dehydration from fluid loss through the wound can lead to organ failure faster than the pain itself suggests.
Can I safely pop a burn blister if it is under tension?
Dermatological consensus is almost universally against the amateur lancing of blisters. That bubble