The Anatomy of a Vascular Illusion: What Actually Is a False Aneurysm?
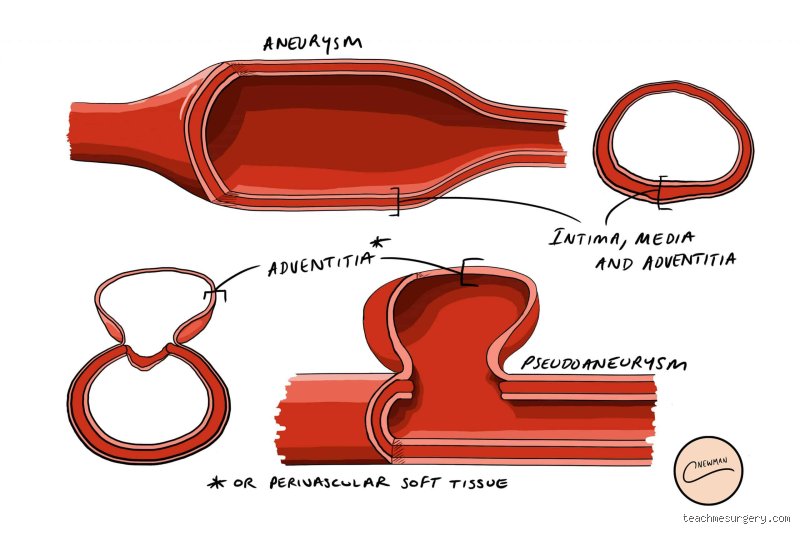
People don't think about this enough, but your arteries are essentially high-pressure plumbing. When a true aneurysm forms, the structural vessel wall weakens and balloons outward, ballooning out like an overinflated tire. A pseudoaneurysm—or false aneurysm—is an entirely different beast altogether. Here, the arterial wall actually tears completely through, letting blood leak into the surrounding tissue where it creates a churning, pulsating pool contained only by a fragile wrapper of clotted blood and fibrous adventitia. Imagine a high-pressure garden hose sprouting a leak, except the water is trapped in a tight pocket of mud just outside the rubber. That is your pseudoaneurysm. It is a ticking clock. Because it lacks the structural support of the three proper arterial layers—the intima, media, and adventitia—the risk of catastrophic rupture is fundamentally higher than what you see in a true arterial dilation. Where it gets tricky is that they often look identical on a cursory ultrasound, masking the true danger beneath a deceptive pulse.
The Femoral Artery Ground Zero: Why Iatrogenic Injuries Dominate
Most of these vascular nightmares do not just happen by chance; we create them. The vast majority of clinical cases occur in the groin, specifically within the common femoral artery, following invasive cardiac catheterizations or angioplasty procedures. Think about the sheer volume of interventional cardiology work done globally. Doctors poke a heavy-gauge needle into a high-pressure artery, run catheters up to the heart, and then pull the lines out, relying on manual compression or a closure device to seal the breach. But what if the closure fails? If the puncture site does not thrombose properly, blood keeps pumping out into the femoral sheath. I watched a case at a municipal hospital in Chicago back in 2024 where an elderly patient developed a massive 4.5-centimeter groin mass just twelve hours after a routine coronary stent placement. The groin turned a deep, terrifying shade of purple, thumping in perfect sync with his heartbeat. That changes everything for a recovery plan. This specific mechanism of injury is known as an iatrogenic pseudoaneurysm, a sterile medical term for an accidental, physician-induced hole in a critical pipeline.
Decoding the Clinical Chaos: When Does the Alarm Bell Ring?
The thing is, identifying this condition before it disintegrates into a hemorrhagic emergency requires a sharp clinical eye. Patients usually notice a painful, throbbing lump near a recent surgical incision or trauma site. But the real diagnosis happens under the skin, where the blood is actively swirling. If a doctor places a stethoscope over the mass, they will often hear a distinct, rhythmic blowing sound—a bruit—caused by the turbulent blood rushing through the narrow neck of the injury. Is every throbbing lump a surgical emergency? Honestly, it's unclear until you get imaging, as many small leaks remain completely silent, buried deep in tissue layers. Yet, when symptoms escalate to skin necrosis or nerve compression, the clinical trajectory shifts instantly. In the lower extremities, a growing pocket of blood can compress the adjacent femoral nerve, triggering a shooting, agonizing pain down the leg that leaves the patient entirely incapacitated.
The Yin-Yang Sign: Looking Through the Diagnostic Lens
To truly understand what we are dealing with, physicians rely heavily on color Doppler ultrasonography. This non-invasive imaging modality is the gold standard for a reason. When the ultrasound technician places the probe over the suspected area, the screen lights up in a chaotic swirl of red and blue. This visual phenomenon is formally called the yin-yang sign, illustrating the blood spinning into the false aneurysm sac during systole and swirling back out into the native artery during diastole. Medical teams use these precise acoustic maps to measure the exact dimensions of the neck and the sac. If the sac diameter exceeds 30 millimeters, or if the patient is on aggressive anticoagulant therapy like warfarin or clopidogrel, the likelihood of spontaneous closure drops to nearly zero. But we're far from it being a simple math problem; the structural stability of that fibrous wall matters just as much as the raw numbers on the screen.
The Triage Protocol: Evaluating the True Necessity of Surgery
We need to talk about the historical bias toward open surgery. For decades, the moment a false aneurysm was detected, surgeons would prep the operating room, slice open the tissue, find the bleeding arterial tear, and stitch it shut with synthetic suture material. It was brutal but effective. Today, we realize that leaping straight to the scalpel for a stable, 1.5-centimeter asymptomatic leak is often an unnecessary risk that exposes vulnerable patients to hospital-acquired infections and prolonged anesthesia. The clinical consensus has evolved dramatically. Modern vascular protocols mandate a strict risk-stratification system based on objective anatomical landmarks. If the neck of the pseudoaneurysm is wide—meaning the channel connecting the artery to the blood pocket is broad—the risk of rupture spikes while the chance of self-healing plummets. Conversely, a long, narrow neck restricts blood flow, acting as a natural brake that encourages thrombus formation inside the cavity. Experts disagree on the exact day-count to wait, but a conservative observation window of 14 to 21 days is frequently deployed for tiny, stable lesions.
When Waiting Becomes Lethal: The Absolute Indications for Surgery
But let us not romanticize watchful waiting; there are lines that, once crossed, mean you must operate immediately. A rapidly expanding hematoma will ruthlessly tear through overlying skin, leading to massive external hemorrhage. Furthermore, if the false aneurysm begins compressing the adjacent deep veins, it can trigger localized deep vein thrombosis, a complication that can easily culminate in a fatal pulmonary embolism. Consider a patient presenting with an infected pseudoaneurysm—often seen in the context of intravenous drug use or contaminated surgical fields—where the bacterial burden dissolves the arterial wall entirely. You cannot watch and wait an infection. In these dire scenarios, conventional open surgery is not just an option; it is the single barrier preventing systemic sepsis and exsanguination. The surgeon must rapidly gain proximal and distal control of the pulsing artery, debride the necrotic, infected tissue, and frequently construct an extra-anatomical bypass using a harvested vein graft to keep the limb alive.
Modern Alternatives: Displacing the Scalpel with Less Invasive Tools
Except that open surgery is no longer the undisputed king of the vascular wing. The advent of ultrasound-guided interventions has completely revolutionized how we approach these dynamic injuries, turning what used to be a two-hour open operation into a ten-minute bedside procedure. The most elegant manifestation of this shift is ultrasound-guided thrombin injection. During this procedure, a clinician inserts a fine needle directly into the center of the pseudoaneurysm sac under continuous, real-time ultrasound visualization. Once the needle tip is perfectly positioned far away from the arterial neck, the physician slowly injects a small dose of bovine or human thrombin—typically around 500 to 1,000 units. Thrombin is an enzyme that instantly converts fibrinogen to fibrin, causing the liquid pool of blood to solidify into a hard clot within seconds. It is a breathtaking transformation to watch on screen; the vibrant blue and red yin-yang swirl vanishes instantly, replaced by a stagnant, grey blanket of thrombosis, while the native artery continues to flow uninterrupted beneath the sealed leak.
The Mechanical Crush: Understanding Ultrasound-Guided Compression
Before thrombin injection gained widespread acceptance in the early 2000s, clinicians relied heavily on a more primitive technique: ultrasound-guided compression therapy. The concept was straightforward yet grueling. A clinician would place the ultrasound transducer directly over the neck of the pseudoaneurysm and press down with immense physical force, manually obliterating the channel connecting the artery to the sac. The goal was to hold this intense pressure for 10-minute cycles, often lasting up to an hour in total, to stop the flow long enough for a clot to form naturally. As a result: patients absolutely hated it. The procedure was notoriously painful, frequently requiring high doses of intravenous sedatives, and it carried a miserable failure rate approaching 30% to 40% in patients who were concurrently taking antiplatelet medications. While it remains a viable fallback option in resource-limited settings where synthetic thrombin is unavailable, it has largely been relegated to the annals of vascular history due to its sheer inefficiency and patient discomfort.
Common Mistakes and Misconceptions Regarding False Aneurysms
The Illusion of the Spontaneous Cure
Many clinicians adopt a passive, wait-and-see attitude because they assume every small hematoma resolves on its own. It is a dangerous gamble. While a minuscule sac under 2 centimeters might thrombase without intervention, larger structural defects simply will not. The problem is that waiting too long allows the sac wall—which lacks true arterial layers—to thin out under relentless systolic pressure. Because of this hemodynamic pounding, an ignored defect can abruptly rupture, transforming a manageable outpatient scenario into a bloody, midnight emergency. Let's be clear: hoping for a miracle closure while ignoring a expanding pulsatile mass is a recipe for clinical disaster.
Confusing True and False Aneurysms
Medical professionals sometimes mistake these disruptive hematomas for true arterial dilations. The distinction matters immensely for your survival. A true aneurysm involves all three layers of the arterial wall, whereas a pseudoaneurysm is merely a contained pocket of blood leaking through a torn vessel. Treating them with the same long-term pharmaceutical regimen is useless. Yet, some practitioners still prescribe standard blood pressure tracking alone, failing to realize that the structural integrity of the tissue has already completely vanished.
Over-Reliance on Physical Palpation
Can you simply feel a pulse and know the exact status of the vascular tear? Absolutely not. Relying solely on manual examinations or the presence of a thrill leads to massive diagnostic failures. Some lesions remain deeply buried under layers of dense scar tissue or fat, masking their standard physical signs. A formal color Doppler ultrasound must always supersede basic physical touch, which explains why blind compression attempts without ultrasound guidance frequently fail or worsen the local arterial damage.
The Hidden Threat: Latent Neurological Compression
When Mass Effect Shadows Vascular Risk
Everyone focuses on the risk of exsanguination. Except that hemorrhage is not the only catastrophic outcome on the table. A growing pseudoaneurysm exerts massive localized mechanical pressure on adjacent anatomical structures. When these expanding blood pockets develop in the femoral or brachial regions, they frequently entrap neighboring peripheral nerves. This chronic compression induces progressive ischemia within the nerve sheath itself, leading to irreversible motor deficits and agonizing neuropathy. Early surgical decompression is often required not because the vessel is about to burst, but because the adjacent nerve is actively dying from starvation.
As a result: delayed intervention risks leaving the patient with a permanent foot drop or a useless, withered hand. (Vascular surgeons sometimes forget that neurological preservation is just as vital as maintaining a strong distal pulse). The issue remains focused on the plumbing, while the delicate electrical wiring of the limb is quietly crushed. Balancing these competing anatomical priorities requires an experienced multidisciplinary approach rather than a narrow, single-specialty focus.
Frequently Asked Questions
Does pseudoaneurysm need surgery if it is under three centimeters?
Not every small vascular defect demands an immediate trip to the operating room. Data indicates that approximately 60% of small pseudoaneurysms under 3 centimeters thrombase spontaneously within four weeks without any aggressive intervention. However, this conservative pathway requires strict ultrasound surveillance every seven days to guarantee the sac is shrinking rather than expanding. If the lesion remains patent after 30 days or causes pain, clinicians typically abandon observation and pivot toward ultrasound-guided thrombin injection, which boasts a 92% success rate for small defects. Therefore, a small size grants you a brief window for observation, but it is never a blanket pass to completely ignore the condition.
What happens if a pseudoaneurysm is left untreated entirely?
Leaving a large vascular leak alone is an invitation to systemic chaos. The thin, fibrous capsule holding the blood back will eventually degrade under the constant force of arterial pressure. Rupture is the most terrifying consequence, leading to massive internal bleeding, rapid hypovolemic shock, and potential loss of limb or life. Furthermore, the turbulent blood flow inside the sac acts as a breeding ground for erratic clots. These thrombi can dislodge at any moment, traveling downstream to block distal arteries and cause acute, limb-threatening ischemia.
How long is the recovery period after undergoing a repair procedure?
The timeline for healing depends entirely on whether your surgeon utilized a minimally invasive approach or standard open reconstruction. Patients undergoing percutaneous thrombin injections or endovascular stenting are frequently discharged within 24 hours, requiring only a few days of restricted physical activity. Conversely, open surgical repair involves a formal incision, tissue dissection, and direct arterial suturing, which demands a 3-day hospital stay. Full functional recovery for open interventions ranges from four to six weeks, assuming no wound complications occur. Patients must avoid heavy lifting during this timeframe to prevent stress on the newly repaired arterial wall.
A Definitive Verdict on Vascular Intervention
We must stop treating vascular leaks as minor inconveniences that might just fade away with time. The data speaks for itself, and the risks of procrastination far outweigh the convenience of avoidance. Prompt objective diagnosis paired with decisive intervention saves limbs and prevents catastrophic systemic failures. Waiting for symptoms to escalate before acting is an outdated, reckless approach to modern patient care. Endovascular covered stents and ultrasound-guided techniques have rendered traditional watch-and-wait strategies largely obsolete for medium to large lesions. In short, when a blood vessel wall breaks, you fix it immediately before the choice is painfully taken out of your hands.