The Anatomy of a False Promise: What Actually Fails When a Pseudoaneurysm Ruptures?
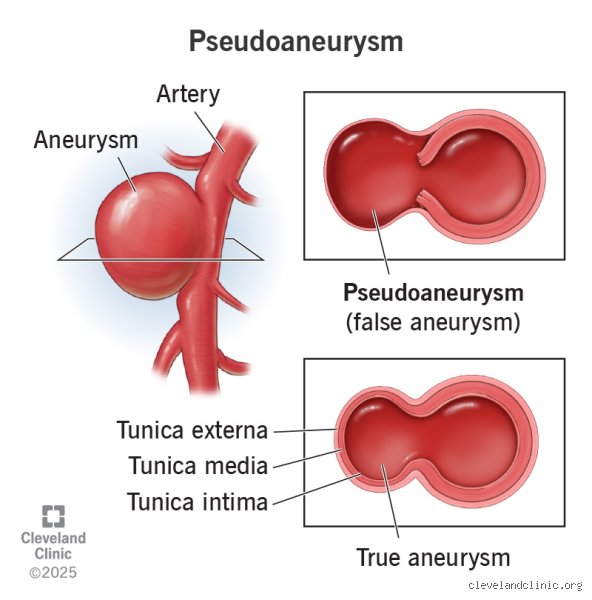
To understand the bleeding mechanics, we need to strip away the textbook sanitized definitions and look at the raw physics of the human vascular system. A true aneurysm expands like an overinflated balloon, keeping its structural integrity intact for years because the muscular media layer, though thinned out, is still trying to hold the line. A pseudoaneurysm skips that entire grace period. The thing is, this structure is born from a literal hole in the vessel, a tear caused by a stray catheter during a percutaneous coronary intervention at a hospital like the Mayo Clinic, a knife wound, or local erosion from a raging infection. Blood punches through the tunica intima and media, pooling outside the vessel footprint, creating what we call a pulsating hematoma.
The Illusion of Containment
People don't think about this enough: the wall of a pseudoaneurysm is an imposter. It is mostly composed of compressed fibrin, platelets, and whatever random connective tissue happens to be adjacent to the injury site. Imagine trying to patch a high-pressure garden hose with nothing but duct tape and wet cardboard; that changes everything regarding how we assess risk. Because there is no real muscular or elastic tissue shielding this pocket, the constant, rhythmic pounding of systolic blood pressure—often exceeding 120 mmHg in hypertensive patients—steadily shears away at the thrombus shell.
When the Shell Crumbles
But why do some hold for weeks while others blow open within hours? The issue remains highly dependent on the neck geometry. A wide neck allows high-velocity arterial jets to constantly destabilize the internal clot, preventing the false sac from organizing into a stable, fibrotic mass. If the internal pressure outpaces the tensile strength of the surrounding inflammatory capsule, the barrier splits. And when that happens, the bleeding is rarely a slow, manageable trickle.
The Cascade of Hemorrhage: Triggers, Flow Dynamics, and Fatal Pressures
When a pseudoaneurysm decides to bleed, the clinical presentation depends entirely on its geography. Take a post-catheterization femoral pseudoaneurysm, which historically occurred in up to 6% of complex interventional procedures before smaller sheath sizes became the norm. If it ruptures superficially, you get a massive, visible hematoma that can track down the thigh, dissecting through fascial planes and trapping liters of blood before anyone even notices a drop in systemic pressure. But what happens if the lesion is hidden deep within the visceral circulation?
The Hidden Catastrophes of Visceral Lesions
A hepatic or splenic pseudoaneurysm, often triggered by a bout of severe acute pancreatitis where digestive enzymes literally eat through the arterial wall, behaves like a phantom. There is no external lump to palpate. Instead, the erosion progresses silently until the pseudoaneurysm ruptures directly into the peritoneal cavity or the pancreatic duct, a terrifying phenomenon known as hemosuccus pancreaticus. Honestly, it's unclear to many junior residents why a patient's hemoglobin is plummeting until the sudden onset of hemorrhagic shock turns the ER upside down. The bleeding here is massive, unyielding, and carries a historical mortality rate that hovers stubbornly around 25% to 40% if surgical or endovascular intervention is delayed by even an hour.
The Role of Sudden Hemodynamic Spikes
Can a simple cough or a sudden movement trigger the hemorrhage? Absolutely, especially in visceral or carotid variants where external mechanical support is negligible. A sudden spike in intrathoracic pressure can abruptly elevate central arterial pressure, creating a transient pressure gradient that the fragile fibrin wall simply cannot withstand. As a result: the containment fails, the pocket decompresses, and the patient begins to bleed out internally.
The Diagnostics of Doom: Spotting the Impending Rupture Before the Deluge
We cannot talk about the bleeding risks without interrogating how we visualize these ticking clocks. The gold standard for initial assessment remains Duplex ultrasonography, which reveals the classic, almost hypnotic yin-yang sign within the false lumen. This swirling red-and-blue pattern represents the blood rushing in during systole and churning back out during diastole through the narrow neck. Yet, ultrasound has its limitations, especially when subcutaneous edema or a massive body mass index obscures the view.
Advanced Imaging and the Signs of Imminent Failure
Where it gets tricky is differentiating a stable, partially thrombosed pseudoaneurysm from one that is actively unraveling. That is where Multidetector Computed Tomography Angiography (CTA) steps in, providing rapid, sub-millimeter isotropic resolution of the vascular architecture. On a CTA scan, a radiologist looks for specific, ominous signs: contrast extravasation, irregular or lobulated sac borders, and the "sentinel clot" sign, which indicates that minor, self-limiting sentinel bleeds have already occurred. I once watched a veteran vascular surgeon look at a 5.5 cm brachial artery pseudoaneurysm on a CTA monitor, point to a tiny, asymmetric outpouching of contrast, and say, "That thing is going to blow before midnight." He was right; we were in the operating room within forty minutes.
Contrasting Realities: Why True Aneurysms and Pseudoaneurysms Part Ways at the Breaking Point
It helps to contrast these lesions with true aneurysms to appreciate the volatile nature of the false variant. A true abdominal aortic aneurysm (AAA) is a chronic disease of aging, matrix metalloproteinases, and atherosclerosis, expanding at a predictable, agonizingly slow rate of roughly 0.3 to 0.5 cm per year. Clinicians have guidelines, like the classic 5.5 cm threshold, before they even consider recommending an elective repair. We have the luxury of time, surveillance, and risk-factor modification.
The Rules of Engagement Do Not Apply Here
With a pseudoaneurysm, we are far from that kind of comfortable predictability. Because the structural integrity is completely compromised from day one, size criteria are notoriously unreliable indicators of stability. A tiny, 1.5 cm pseudoaneurysm of the gastroduodenal artery can rupture with the exact same lethal velocity as a massive femoral lesion. Except that the femoral lesion is constrained by the tough fascia lata, whereas the visceral one has nothing but the compliant, easily displaced abdominal organs to hold it back. This absence of a predictable growth-to-rupture ratio means that any pseudoaneurysm, regardless of its dimensions, must be viewed as an unstable lesion demanding immediate clinical respect and, more often than not, definitive closure.
Common Blunders and Misunderstandings
The Illusion of the Vascular Wall
Many clinicians mistake a pseudoaneurysm for a true aneurysm, assuming a layered, structurally sound vessel wall protects the patient. Let's be clear: a false aneurysm possesses no true arterial tunic. It is merely a contained hematoma bounded by adventitia or perivascular soft tissue. Because this fragile barrier lacks muscular or elastic fibers, it remains highly unstable. Believing that a lack of systemic symptoms equates to stability is a dangerous gamble. The structural integrity is inherently compromised from day one.
Misinterpreting the Absence of a Bruit
Does a pseudoaneurysm bleed if you cannot hear it? Absolutely. Doctors often rely heavily on physical examination hallmarks like a palpable thrill or an audible machinery bruit. Yet, these classic signs disappear entirely when a clot occludes the narrow communicating neck. This false reassurance leads to delayed diagnostic imaging. Relying solely on your stethoscope in these scenarios invites disaster, especially when evaluating post-catheterization femoral access sites where thrombus accumulation masks active turbulence.
The Watchful Waiting Trap
Waiting for spontaneous resolution in high-risk zones is another frequent misstep. While small cavities under two centimeters occasionally thrombose without intervention, larger lesions rarely do. Forcing a conservative strategy on a expanding pulsatile mass is reckless. It ignores the compounding hemodynamic shear stress. The problem is that delaying a definitive thrombin injection or ultrasound-guided compression simply gives the lesion more time to rupture into adjacent anatomical compartments.
The Hidden Impact of Biomechanical Shear Stress
How Local Turbulence Dictates Rupture Risk
We often focus exclusively on the absolute diameter of the vascular sac when calculating danger. Except that diameter is a deceptive metric. The real culprit behind sudden degradation is the intra-luminal jet velocity spinning through the neck. This localized vortex exerts massive destructive force against the friable fibrin wall. High systolic blood pressure exasperates this swirling motion, which explains why uncontrolled systemic hypertension accelerates rupture timelines exponentially. Have you ever seen a fabric seam rip under a pressure washer? That is precisely what occurs at the cellular level inside the cavity. As a result: sudden, catastrophic failure happens without any warning size increase. Investigators must utilize color Doppler quantification to analyze these velocity vectors rather than just measuring the boundaries of the sac. It is an imperfect science, but prioritizing flow dynamics over mere geometry saves lives.
Frequently Asked Questions
What percentage of iatrogenic pseudoaneurysms actually rupture if left untreated?
Data indicates that approximately 2% to 6% of all iatrogenic arterial injuries progress directly to acute, uncontrollable hemorrhage if entirely ignored. However, this statistical probability spikes dramatically to nearly 35% when the lesion exceeds a diameter threshold of three centimeters. Medical literature confirms that radial artery false aneurysms bleed faster than deep femoral ones due to minimal surrounding tissue support. In short, leaving these arterial disruptions to heal on their own is an unjustifiable clinical gamble.
Can a chronic pseudoaneurysm remain silent for years before bleeding?
Yes, an encapsulated hematoma can theoretically remain dormant for months or even years if it develops a thick fibrous capsule. But the issue remains that any subsequent blunt trauma, local infection, or sudden spike in intra-arterial pressure can destabilize this delicate balance. Once the protective fibrous matrix degrades, the lesion behaves exactly like an acute vascular rupture. Over time, erosion into adjacent structures like bones or nerves typically forces a symptomatic presentation before complete exsanguination occurs.
How do doctors definitively differentiate between a hematoma and an active pseudoaneurysm?
Distinguishing between these two conditions requires a color flow Doppler ultrasound to identify the characteristic yin-yang sign within the lumen. A standard hematoma presents as a stagnant, avascular fluid collection that exhibits no internal color signals during a cardiac cycle. Conversely, the false aneurysm displays active, bidirectional flow through the communicating neck. Because contrast-enhanced computed tomography angiography provides definitive visualization, it remains the gold standard for complex anatomical regions like the thoracic or abdominal aorta.
A Definitive Stance on Vascular Vigilance
We must abandon the passive complacency that characterizes the management of modern vascular complications. Waiting for a pulsatile mass to display overt signs of failure before intervening is an archaic approach to patient care. The data clearly shows that early percutaneous thrombin injection minimizes morbidity far better than delayed surgical reconstruction. Every single suspected arterial wall disruption demands immediate, aggressive imaging verification regardless of how stable the patient appears on paper. Do you really want to wait for sudden hemorrhagic shock to confirm your diagnosis? Our collective clinical mindset needs to shift from reactive observation to proactive, ultrasound-guided elimination. Ultimately, treating these ticking time bombs with anything less than total therapeutic urgency is an insult to modern preventative medicine.