The Anatomy of 140/90: What These Numbers Are Actually Doing to Your Body
Blood pressure isn't a static figure; it’s a fluid, rhythmic conversation between your heart and your peripheral resistance. When that gauge hits 140/90, we are looking at the systolic pressure (the 140) and the diastolic pressure (the 90). The former represents the force when the heart beats, while the latter reflects the pressure in the arteries when the heart rests between beats. People don't think about this enough, but that resting phase is where the coronary arteries actually get their own blood supply. If the 90 becomes a 100 or a 110, that window of recovery for the cardiac muscle starts to slam shut. It’s a mechanical grind that, over years, turns supple vessels into stiff, scarred pipes.
Breaking Down Stage 1 Hypertension Guidelines
The American Heart Association redefined these goalposts back in 2017, shifting the "high" label from 140/90 down to 130/80. Why? Because the data from the SPRINT trial showed that lower targets significantly reduced cardiovascular events. Yet, here is where it gets tricky: clinical guidelines are one thing, but your personal physiology is another. If your "normal" is 110/70, a jump to 140/90 is a massive internal shift that might make you feel jittery or flushed. But if you've lived at 135/85 for a decade, your body has likely compensated for that load. The issue remains that 140/90 is the "borderline" zone. It’s the medical equivalent of driving a car with the RPMs perpetually in the red—you won't explode today, but you're definitely burning out the engine faster than necessary.
The Difference Between a Spike and a Trend
Did you just drink a double espresso? Are you arguing with a relative about politics? Because those factors can easily kick a healthy person into the 140/90 range for an hour or two. We call this labile hypertension. It is transient. And frankly, the medical community is divided on how much these "spikes" actually matter in the long run compared to a steady, unrelenting baseline. Some experts argue the peaks do the most damage to the delicate endothelial lining, while others insist it's the average over 24 hours that predicts a stroke. I tend to lean toward the trend; one bad reading is a fluke, but three bad readings in a week is a pattern that requires a prescription pad or a radical lifestyle overhaul.
When 140/90 Becomes a True Medical Emergency: Red Flags to Watch For
Context is everything in medicine. If you are a 25-year-old athlete and you see 140/90 after a sprint, you're fine. However, if you are 32 weeks pregnant, that exact same number is a potential siren for preeclampsia, a condition that can escalate into seizures or organ failure within hours. As a result: we cannot look at the digits in a vacuum. A blood pressure of 140/90 accompanied by a "thunderclap" headache—the kind that feels like a literal explosion in your skull—demands an immediate CT scan to rule out a subarachnoid hemorrhage. It's rare, sure, but ignoring it is a gamble no one should take.
Hypertensive Urgency vs. Hypertensive Crisis
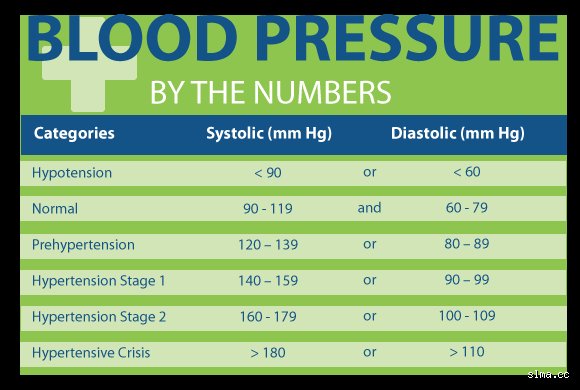
We need to distinguish between these two because the terminology is often used interchangeably by patients, which leads to unnecessary ER overcrowding. A hypertensive crisis generally involves readings above 180/120. That is the "danger zone" where the pressure is so high it can cause the aorta to tear or the brain to swell. 140/90 is nowhere near that. Yet, if that 140/90 is paired with shortness of breath or pain radiating down your left arm, the blood pressure itself isn't the problem—it’s a symptom of an ongoing myocardial infarction. That changes everything. In that scenario, you aren't going to the hospital for the BP; you're going because your heart tissue is actively dying. But without those specific symptoms? You’re likely just looking at a slow-burning chronic condition.
The Role of Target Organ Damage
The kidneys are the silent victims here. They are essentially bundles of microscopic filters called nephrons that are incredibly sensitive to pressure changes. When the "90" in your blood pressure stays high, it hammers away at these filters. Over years, this leads to chronic kidney disease (CKD), which often has zero symptoms until you're staring at a dialysis machine. But let's be honest, you aren't going to feel your kidneys failing at 140/90. Which explains why doctors are so insistent on treating it early. It’s about preventing a catastrophic failure in 2045, not necessarily in 2026. Is it frustrating to take a pill for something you can't feel? Absolutely. But the math of human biology is unforgiving.
The Physiology of Pressure: Why 140/90 Isn't Just a Number
Your blood vessels are not just static tubes; they are dynamic organs that produce hormones and respond to stress. At 140/90, the sheer stress—that’s the actual physical friction of blood scraping against the vessel walls—is high enough to cause microscopic tears. This is where the trouble starts. Cholesterol doesn't just stick to healthy walls; it gets trapped in these tears, forming atherosclerotic plaques. Think of it like a smooth highway versus one with potholes. Once the potholes appear, the debris starts to pile up. Hence, the 140/90 reading is the moment the potholes start forming. If you catch it now, you can "pave" over the damage with diet, exercise, or medication. If you wait until it's 160/100, the road is already crumbling.
The Impact of Sodium and the Renin-Angiotensin System
Most people think salt just makes you thirsty. The reality is far more complex and involves a hormonal cascade called the Renin-Angiotensin-Aldosterone System (RAAS). When you consume excess sodium, your body retains water to dilute it, increasing the total volume of fluid in your pipes. More fluid in the same sized pipe equals higher pressure. But some people are "salt-sensitive," meaning their RAAS is hyper-reactive. For them, a single salty meal at a local bistro in New York or London can swing their pressure from 125/80 to 145/95 overnight. It’s a temporary bloat, but for the vascular system, it’s like a flash flood. But does it warrant a hospital stay? Hardly. It warrants a glass of water and a salad.
Comparing 140/90 to Higher Intervals: The Risk Gradient
To understand the risk of 140/90, we have to look at what lies beyond. At 160/100 (Stage 2), the risk of a cardiovascular event doubles compared to someone with optimal pressure. At 140/90, the risk is elevated, but it’s manageable. Statistically, according to the Framingham Heart Study, a long-term project that has tracked thousands of participants since 1948, individuals in this range have a significantly higher lifetime risk of developing heart failure. But—and this is a big "but"—that risk is mitigated almost entirely if the pressure is brought back under control within a year or two of onset. It isn't a death sentence; it's a window of opportunity.
Home Monitoring vs. The White Coat Effect
There is a massive phenomenon known as White Coat Hypertension where patients' blood pressure spikes purely because they are in a clinical setting. I have seen patients hit 150/95 in my office, only to go home and average 118/75 on their own cuff. This is why a single 140/90 reading at a doctor's office or hospital is notoriously unreliable. To get a real sense of what’s happening, you need Ambulatory Blood Pressure Monitoring (ABPM). This involves wearing a cuff for 24 hours that takes readings every 30 minutes. In short, your 140/90 might not even be your real blood pressure. It might just be your nervous system reacting to the smell of antiseptic and the sight of a lab coat.
The "Silent Killer" Moniker: Hyperbole or Fact?
We call hypertension the "silent killer" because it rarely presents with obvious symptoms like a cough or a rash. This creates a dangerous complacency. If 140/90 made your skin turn bright purple, people would be beating down the doors of the ER. Instead, it just quietly thins the walls of your heart, a process called left ventricular hypertrophy. The heart muscle gets thicker and stiffer to push against the resistance. Eventually, it loses the ability to pump effectively. Honestly, it's unclear why some people can tolerate 140/90 for decades without much issue while others suffer a stroke at 145/92. Genetics plays a massive, often unfair role here. But until we can map every single person's genetic vulnerability, the 140/90 cutoff remains our best line of defense.
Myth-Busting: Why Most People Get It Wrong
The "Silent Killer" Isn't Just a Cliche
Many patients walk into the clinic convinced that a lack of headaches or dizziness means they are safe. The problem is, your vasculature is remarkably resilient right up until the moment it isn't. People often assume that a reading of 140/90 mmHg will feel like something, perhaps a buzzing in the ears or a flushed face. But it doesn't. You might feel spectacular while your arterial walls undergo micro-tears that invite plaque buildup. Waiting for symptoms before asking do I need to go to hospital if my BP is 140-90 is like waiting for your engine to explode before checking the oil. Unless you are experiencing chest pain or neurological deficits, the ER is the wrong destination, yet the ignorance regarding the lack of physical feedback remains a top-tier medical hurdle.
The Coffee and Stress Scapegoat
"I just had an espresso" or "It was a stressful drive here" are the most frequent excuses heard in primary care. While it is true that caffeine can spike systolic pressure by 10 to 15 points, chronic hypertension is not born from a single bean. Let's be clear: a healthy cardiovascular system should recover its baseline rapidly after a stressor. If your numbers stay parked at 140/90 mmHg for two hours after a stressful meeting, the issue remains your systemic vascular resistance, not the meeting itself. We often see patients dismiss these "situational" spikes for years. Consequently, they miss the narrow window for lifestyle intervention before the kidneys begin to stiffen under the relentless pressure of stage 2 hypertension. Are you really going to bet your longevity on a venti latte being the sole culprit?
The Circadian Rhythm: An Expert Secret
The Dangerous Mystery of the Non-Dipper
Most clinicians focus on the office reading, but the real data hides in your sleep. Normally, blood pressure drops by 10% to 20% during the night, a phenomenon known as dipping. Except that some individuals are non-dippers, meaning their nocturnal blood pressure stays elevated or even rises. This is a massive red flag. If your daytime average is 140/90 mmHg, but it never drops while you sleep, your 24-hour pressure load is significantly higher than someone with the same daytime average who "dips" properly. Research indicates that non-dippers have a 2.5 times higher risk of stroke and heart failure. This is why we increasingly advocate for Ambulatory Blood Pressure Monitoring (ABPM), which involves wearing a cuff for a full day and night to catch the patterns that a single office visit simply cannot reveal.
Frequently Asked Questions
Is it normal for the top number to be high but the bottom to be low?
This condition is known as Isolated Systolic Hypertension and it is incredibly common in adults over the age of 60. As we age, our large arteries lose their elasticity and become stiff, which explains why the systolic pressure climbs while the diastolic stays within normal ranges like 70 or 80 mmHg. Data from the Framingham Heart Study suggests that for older populations, the top number is a far more potent predictor of cardiovascular events than the bottom number. You still need medical management if the gap between the two numbers, known as pulse pressure, becomes excessively wide. But do not panic if your 140/90 reading occasionally looks more like 150/75, as both require a conversation with your GP rather than an emergency siren.
Should I start taking aspirin if I see a 140/90 reading?
Absolutely do not start a daily aspirin regimen without a specific prescription from a cardiologist. While aspirin was once the gold standard for prevention, modern guidelines from the USPSTF have shifted significantly due to the high risk of internal bleeding. Taking aspirin for a 140/90 mmHg reading without knowing your 10-year ASCVD (Atherosclerotic Cardiovascular Disease) risk score is dangerous. In short, aspirin thins the blood but it does not lower