The Anatomy of a Lie: Understanding the Structural Failure of the Arterial Wall
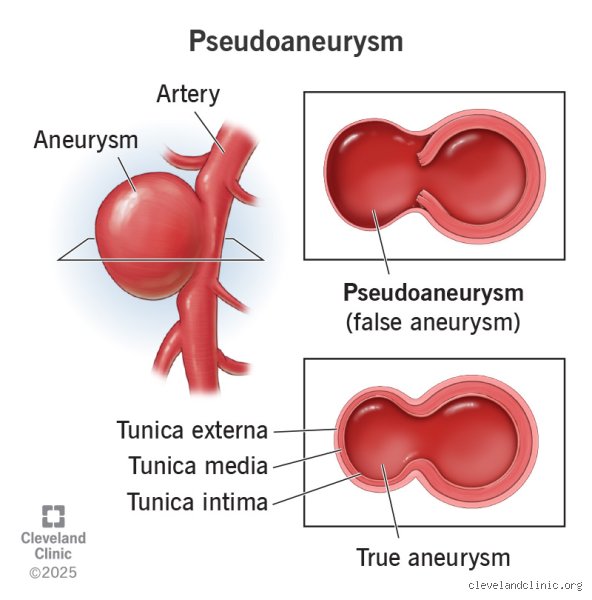
Arteries are impressive pieces of biological engineering, designed to withstand the rhythmic hammer of systolic pressure day in and day out for decades. They are built in three distinct layers, a trinity of tissue that ensures blood stays where it belongs. When we talk about a true aneurysm, such as the classic abdominal aortic aneurysm (AAA), we are describing a scenario where all three layers have become stretched and thin. Think of it like an old garden hose that develops a soft spot; the rubber is still there, but it is expanded beyond its original diameter. This permanent dilation must usually exceed 50% of the normal vessel diameter to earn the clinical label. It is a slow, degenerative process, often whispered through the body over years without a single outward sign until the moment of crisis.
The Triple-Layer Defense System
The intima, the media, and the adventitia—these aren't just fancy Latin names but the difference between life and death. The tunica media is the powerhouse, packed with elastic fibers and smooth muscle cells that allow the vessel to recoil. In a true aneurysm, this layer loses its snap. But here is where it gets tricky: in a pseudoaneurysm, the tunica media has been completely breached. There is no wall left. Instead, the blood is held in place by the adventitia (the outermost layer) or, more commonly, by the sheer pressure of the muscles and fascia surrounding the leak. We are far from the structural continuity of a healthy vessel. It’s more like a pothole that has been covered with a piece of plywood—it might hold for a moment, but the foundation is fundamentally broken.
Where the Trouble Starts: The Diverse Causes of False Aneurysms in Modern Medicine
If true aneurysms are the result of the slow erosion of time—atherosclerosis, genetics, or chronic hypertension—pseudoaneurysms are the children of trauma. They are sudden. They are violent. Most often today, they are the unintended consequence of the very medical miracles meant to save us. Since the rise of interventional cardiology in the late 20th century, the incidence of iatrogenic pseudoaneurysms has climbed. When a cardiologist threads a catheter through the femoral artery to clear a blockage in the heart, they leave a hole. Usually, that hole heals perfectly. Sometimes, however, the seal fails. The blood escapes, swirling in a pocket outside the artery, creating a pulsatile mass that can be felt under the skin. Data suggests that iatrogenic injuries account for nearly 70% to 80% of pseudoaneurysms seen in urban trauma centers today.
The Impact of Blunt and Penetrating Trauma
Outside the sterile environment of a cardiac cath lab, the world is a dangerous place for arteries. A knife wound or a high-velocity car accident can partially transect a vessel. Because the hole is small and the surrounding tissue is tight, the patient doesn't bleed out immediately. Instead, a pulsating hematoma forms. This is the classic presentation of a pseudoaneurysm. Interestingly, clinicians often see these in the brachial artery of intravenous drug users or the femoral arteries of patients who have undergone recent orthopedic surgery. People don't think about this enough, but even a misplaced biopsy needle can initiate this cascade. It doesn't take much to disrupt the delicate pressure balance of the circulatory system. And that changes everything for the surgeon who has to fix it.
Infection and the Mycotic Variant
Then there is the dark horse of the category: the mycotic pseudoaneurysm. This has nothing to do with mushrooms, despite the name. It occurs when a bacterial infection, often from Staphylococcus aureus or Salmonella, eats a hole through the arterial wall from the inside out. This was a death sentence in the pre-antibiotic era. Even now, with the best drugs available, the mortality rate for an infected pseudoaneurysm remains stubbornly high, sometimes exceeding 40% in certain aortic locations. I find it fascinating that the body's immune response can be so aggressive that it literally dissolves the very pipes keeping it alive. It’s a civil war at the microscopic level.
The Diagnostic Dilemma: Seeing Past the Surface with Advanced Imaging
You cannot tell the difference between a true and false aneurysm just by looking at the patient's skin. Both might present as a throbbing lump. Both might cause pain. To find the truth, we have to look deeper. The gold standard for initial screening is the Color Doppler Ultrasound. This isn't just about taking a picture; it's about watching the physics of blood flow in real-time. In a pseudoaneurysm, radiologists look for the "yin-yang sign." This is a swirling pattern of red and blue color flow within the pocket, representing blood entering and leaving the hematoma through a narrow neck. It’s a beautiful, hypnotic image on the screen, but it’s an omen of a structural failure that requires immediate attention.
Visualizing the Neck of the Leak
The "neck" is the smoking gun. It is the literal channel connecting the artery to the false sac. In a true aneurysm, there is no neck because the entire vessel is dilated. Identifying this narrow passage is the thing is that allows a doctor to differentiate between the two. If the neck is long and thin, there is a better chance the pseudoaneurysm will clot off on its own or respond to ultrasound-guided thrombin injection. But if the neck is wide—say, over 1 centimeter in diameter—the risk of the thrombin leaking back into the main artery and causing a stroke or limb ischemia becomes too high. At that point, the conversation shifts from a simple bedside procedure to a high-stakes surgical repair.
The Evolution of Treatment: From Cold Steel to Chemical Closures
The issue remains that we are dealing with a ticking time bomb. Because a pseudoaneurysm lacks a real wall, its risk of rupture is significantly higher than that of a true aneurysm of the same size. Historically, surgeons had to "cut to cure," opening the limb or the abdomen to manually stitch the hole. It was a messy, risky business. Yet, the landscape changed in 1991 when researchers began experimenting with ultrasound-guided compression. It was a brutal technique—literally leaning on the patient's groin with a transducer for 20 to 60 minutes to force the leak to shut. It was painful for the patient and exhausting for the technician, but it worked in about 75% of cases. Thankfully, we have moved beyond such primitive methods for most patients.
The Rise of Thrombin Injection
Today, the most common fix is elegant and terrifyingly simple. A doctor uses a fine needle to inject bovine thrombin directly into the pseudoaneurysm sac. Thrombin is a clotting enzyme; it turns the liquid blood into a solid plug in seconds. The transformation is nearly instantaneous. One moment, the screen shows the swirling yin-yang of turbulent flow; the next, the screen goes grey and still. It is one of the few things in medicine that offers such immediate gratification. However, experts disagree on whether this should be the first line of defense for everyone. In cases of arterial infection, injecting thrombin is like putting a band-aid on a fire—it doesn't address the underlying destruction of the vessel wall and can actually trap bacteria, leading to a massive abscess. In short, the "easy fix" isn't always the right one. We have to be more discerning than that.
Catastrophic Confusion: Debunking Prevailing Misconceptions
The medical community often treats the word aneurysm as a monolithic label, but this linguistic laziness creates a dangerous diagnostic fog. One of the most frequent errors involves the assumption that a pulsatile mass must be an arterial dilation. It is not always so. If you poke a hole in a garden hose and cover it with duct tape, the bulge you see is not the hose expanding. It is a leak under pressure. In the human body, this leak is the false aneurysm, yet many practitioners still mistakenly document it as a permanent structural failure of the vessel wall. Let's be clear: the problem is that treating a leak like a stretch can lead to surgical disasters.
The Myth of Spontaneous Healing
We often hear that small hematomas simply vanish. While a tiny iatrogenic pseudoaneurysm under two centimeters might occasionally thrombose on its own, banking on this is a reckless gamble. Expecting a high-pressure arterial jet to just stop because of optimism is medically naive. Recent studies indicate that roughly 30 percent of untreated post-catheterization femoral leaks fail to resolve without intervention. But waiting too long invites the specter of skin necrosis or nerve compression. The tissue simply cannot handle the constant thumping of blood against a makeshift wall of fibrin and inflammatory debris forever. Why would we assume a hematoma has the structural integrity of a healthy intima?