The Anatomy of Absence: What Stays and What Goes During Surgery
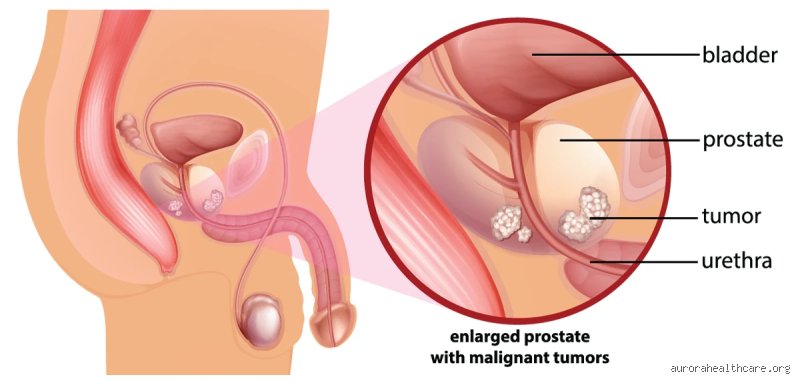
The prostate is not some isolated marble sitting in a void; it is a walnut-sized traffic hub where the reproductive and urinary systems collide. When a surgeon performs a radical prostatectomy—whether it is the da Vinci robotic-assisted method popularized in the early 2000s or the traditional open approach—they are not just removing a gland. They are re-routing plumbing. Imagine a busy intersection where one day, the city decides to remove the central roundabout and replace it with a narrow, straight pipe. Because the prostate sits directly beneath the bladder and wraps around the urethra, its removal leaves a gap. To fix this, the surgeon must pull the bladder neck down and stitch it directly to the remaining urethra. This new connection is known as the vesicourethral anastomosis.
The Disruption of the Pelvic Floor Architecture
People don't think about this enough, but the prostate actually provides structural support. It acts as a physical buffer for the bladder. Once it is gone, the surrounding ligaments and the levator ani muscles have to compensate for the missing mass. Have you ever wondered why some men leak when they sneeze after surgery? It’s because the internal urinary sphincter, which lived inside the prostate, is now in a medical waste bin. Now, the entire burden of continence falls on the external sphincter, a tiny ring of muscle that was never meant to work 24/7 without help. This isn't just a "muscle issue"—it is a fundamental change in the geometry of the male pelvis.
The Fate of the Seminal Vesicles and Vas Deferens
During the procedure, specifically in cases of adenocarcinoma, surgeons typically remove the seminal vesicles as well. These are the small pouches that store the fluid that makes up the bulk of semen. And because the vas deferens—the tubes that carry sperm from the testes—are severed and tied off, the path is permanently blocked. The testicles keep producing sperm, yet there is nowhere for them to go. They are simply reabsorbed by the body, a process that is entirely harmless but psychologically jarring for many. We’re far from the days where this was considered a "minor" side effect; it is a total reproductive shutdown.
The Nerve-Sparing Dilemma: The Fight for Erectile Function
The issue remains that the nerves responsible for erections, the cavernous nerves, are essentially "wallpapered" onto the sides of the prostate. They are microscopic, translucent, and incredibly fragile. Even with the highest-precision robotics, the heat from cautery or the slight traction used to move the gland can cause what we call neuropraxia—a fancy term for the nerves being stunned into a coma. In a "nerve-sparing" surgery, the goal is to peel these fibers away like a sticker from a sheet of paper. But honestly, it’s unclear sometimes if "sparing" them on the operating table translates to function in the bedroom six months later.
Blood Flow and the Threat of Penile Atrophy
If the nerves are damaged, the penis doesn't get its nightly "maintenance" erections—those involuntary events during REM sleep that keep the tissue oxygenated. Without these, the smooth muscle can begin to scar, a process called fibrosis. This explains why many urologists at clinics like the Mayo Clinic or Johns Hopkins now push for "penile rehabilitation" within weeks of the catheter coming out. They use PDE5 inhibitors like sildenafil or vacuum erection devices to force blood into the area. It is a race against time. If the tissue stays dormant for too long, the physical structure of the penis can actually change, leading to a noticeable loss in length or girth.
The Mystery of the "Dry Orgasm"
One of the strangest things for men to wrap their heads around is the anejaculatory orgasm. You can still feel the climax, because that is a neurological event controlled by the brain and the pudendal nerve, which is usually untouched. Yet, nothing comes out. The sensation is different—some describe it as "shorter" or "less intense"—while others find it a relief. But that changes everything about the intimacy experience. It is a ghostly sensation, a phantom limb of the reproductive system. Which explains why the psychological adjustment is often more grueling than the physical healing of the internal stitches.
Urinary Dynamics and the Relentless Bladder
In the immediate aftermath of having the prostate removed, the bladder is basically a confused organ. It spent years pushing against the resistance of the prostate; now, suddenly, that resistance is zero. This leads to detrusor overactivity. The bladder spasms, feeling "full" when it only holds an ounce of fluid. Most patients leave the hospital with a Foley catheter in place for 7 to 14 days to allow the new junction between the bladder and urethra to water-tighten. Once that tube comes out, the real test of the external sphincter begins.
The 90-Percent Rule and Recovery Timelines
Statistics show that while roughly 90% of men eventually regain "social continence" (using one or fewer pads per day) within a year, the journey there is a vertical climb. In a study of 1,000 patients, nearly 40% experienced significant leakage at the three-month mark. It’s not just about doing Kegels; it’s about the striated urethral sphincter thickening over time to handle the new pressure. Yet, some men never fully dry up, especially if they had high-grade tumors that required wider surgical margins. I believe we often undersell the "leaky" phase to patients to keep their spirits up, but the reality is much messier than the brochures suggest.
Comparing Radical Surgery to Focal Alternatives
The standard of care for decades has been the "take it all" approach, but we are seeing a shift. Focal therapies, like HIFU (High-Intensity Focused Ultrasound) or cryotherapy, try to zap only the tumor, leaving the rest of the prostate intact. The difference is night and day regarding side effects. Where a radical prostatectomy removes the entire engine, focal therapy tries to just replace a spark plug. As a result: the recovery is faster, and the nerves are rarely touched. Except that focal therapy isn't for everyone; if the cancer is "multfocal" or aggressive, leaving any prostate tissue behind is like leaving a smoldering coal in a dry forest. Hence, the "gold standard" remains the removal, despite the heavy physiological tax it levies on the male body.
Common traps and urban legends regarding radical prostatectomy
The myth of immediate systemic failure
Many patients walk into the operating theater convinced that the moment the prostate is removed, their entire hormonal ecosystem will collapse into a heap of dust. Let's be clear: your testicles, not your prostate, are the primary engines of testosterone production. Removing the gland does not trigger a sudden drop in androgen levels or transform your metabolic profile into something unrecognizable overnight. The problem is that we often conflate plumbing with chemistry. While the seminal vesicles are typically excised alongside the prostate—leading to a definitive end to ejaculate volume—your libido remains anchored to your endocrine system. But why do men report feeling "different" if the hormones are stable? Psychological shock and the trauma of surgery play a massive role that clinical charts often ignore. Because the nerves controlling erections sit like delicate spiderwebs on the surface of the gland, their temporary (or permanent) trauma is what creates the illusion of lost "manhood."
Misunderstanding the timeline of urinary control
Expectation is a cruel mistress. You might think that once the catheter is pulled out, you will instantly regain the bladder control of a twenty-year-old athlete. It doesn't work that way. The internal sphincter is gone. As a result: the external urethral sphincter must now perform a solo act for which it was never fully trained. Statistics show that while 90% of men achieve social continence within one year, the first three months are often a soggy reality check. Do not mistake the initial leakage for a permanent failure of the procedure. It is a muscular retraining period. Ironically, many men spend thousands on supplements for "prostate health" after the organ is already in a pathology lab, which explains why education is often more valuable than the surgery itself.
The silent shift in pelvic floor mechanics
The forgotten role of the levator ani
What happens to a man's body when the prostate is removed involves a structural vacancy that the surrounding tissues must reconcile. Most surgeons focus on the margins and the oncology, yet the levator ani muscle group is the unsung hero of your post-operative life. When the "spacer" that was your prostate is vacated, the bladder neck is pulled down to the urethra in an anastomosis. This repositioning changes the angle of your pelvic floor. Which explains why pelvic floor physical therapy (PFPT) is not just a suggestion but a requirement for those who want to avoid wearing pads forever. The issue remains that we treat the surgery as an isolated event rather than a total renovation of the lower torso. You are literally relearning how to hold tension in a void. (And yes, it feels as strange as it sounds). Expert advice suggests starting these exercises months before the scalpel ever touches your skin to build what we call "functional reserve."
Frequently Asked Questions
Does prostate removal significantly shorten the length of the penis?
It is a jarring reality that many clinical studies, including those published in the Journal of Urology, indicate an average reduction of 0.5 to 2 centimeters in stretched penile length following surgery. This occurs primarily because the urethra is shortened when it is reattached to the bladder, and the lack of nocturnal erections leads to cavernosal fibrosis or tissue shrinkage. Data suggests that nearly 68% of men notice some degree of shortening within the first year post-prostatectomy. Using a vacuum erection device (VED) as part of a penile rehabilitation protocol can mitigate this loss by forcing oxygenated blood into the tissues. We cannot ignore that structural changes are the trade-off for oncological safety.
How soon can I return to sexual activity after the procedure?
Most surgical teams cleared patients for light physical activity after six weeks, but sexual intimacy often requires a more nuanced "green light" based on healing at the vesicourethral anastomosis. The problem is not the desire, but the mechanical integrity of the internal sutures which need roughly 45 to 60 days to withstand the pressure of climax. While you can achieve a "dry orgasm" as soon as the catheter discomfort fades, the nerve-sparing recovery usually takes 6 to 18 months to produce a functional erection. But what if you don't want to wait that long? Many specialists prescribe low-dose PDE5 inhibitors like Tadalafil daily starting just weeks after surgery to keep the vascular pathways open and responsive.
Is the risk of inguinal hernia higher after this specific surgery?
Recent longitudinal data indicates that men undergoing radical prostatectomy have a 7% to 20% risk of developing an inguinal hernia within the first two years, which is significantly higher than the general male population. This is likely due to the disruption of the transversalis fascia during the pelvic dissection or the scarring that occurs around the internal inguinal ring. The issue remains a point of debate among laparoscopic versus robotic surgeons, yet the statistical trend is undeniable across all modalities. Patients should be vigilant for bulges in the groin area when coughing or lifting heavy objects during their first year of recovery. Is it possible that the cure for one ailment sets the stage for a minor structural breakdown elsewhere?
The harsh reality of the post-prostate era
We need to stop pretending that what happens to a man's body when the prostate is removed is a simple "unplug and play" scenario. It is a visceral transformation. You are trading a biological ticking time bomb for a lifetime of vigilant maintenance and mechanical adaptations. This is not a failure of medicine; it is the price of survival in a body that was never designed to outlive its own cellular mutations. I take the stand that we do a regular disservice to men by over-sanitizing the aftermath of this surgery. The anatomic void left behind is both literal and figurative, demanding a psychological grit that no pelvic exercise can fully provide. In short, the surgery saves the life, but the man must painstakingly rebuild the lifestyle from the wreckage of his former physiology.