The Anatomy of Agony: Why Pancreatitis Is One of the Most Painful Biological Crises
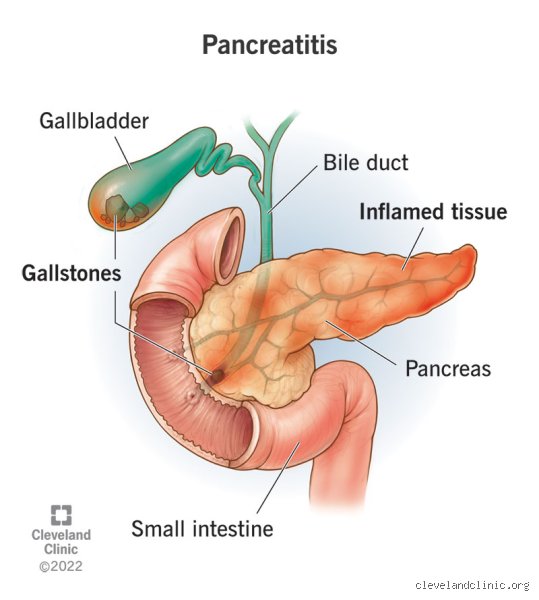
To grasp the sheer ferocity of this condition, we have to look at a modest, six-inch organ tucked quietly behind the stomach. The pancreas is an absolute workhorse, pulling double duty as both an endocrine regulator and an exocrine powerhouse that churns out incredibly potent digestive enzymes like trypsin, chymotrypsin, and lipase. Under normal circumstances, these chemical scalpels remain safely deactivated until they journey into the duodenum. But when the system malfunctions, everything changes.
The Nightmare of Autodigestion
Imagine those highly destructive enzymes activating prematurely while still trapped inside the delicate pancreatic parenchyma. That is the grim reality of acute pancreatic autodigestion, a process where the organ literally begins to dissolve itself. This internal chemical warfare induces massive, localized tissue necrosis. But why does it hurt so intensely? The pancreas shares an intimate, crowded anatomical neighborhood with the celiac plexus—a dense, highly sensitive network of nerves that routes pain signals directly to the brain. When inflammatory fluids, cell debris, and rogue enzymes breach the pancreatic capsule, they bathe these nerve fibers in a highly toxic, corrosive cocktail, causing a relentless, unyielding firing of nociceptors that normal pain medication can barely touch.
The Dreaded Band-Like Radiation
And then comes the structural trap. Because of the retroperitoneal positioning of the pancreas, the swelling presses inexorably backward against the posterior abdominal wall. This explains why a staggering 50% to 70% of patients describe the sensation not just as an abdominal cramp, but as a horrific, boring iron band wrapping around their torso and piercing straight into their lower thoracic vertebrae. You cannot sit up, you cannot lie flat, and curling into a tight fetal position on a cold hospital floor often becomes the only semi-tolerable posture available.
Decoding the True Scale of Pancreatic Inflammation Severity
Medical professionals frequently utilize standardized metrics like the Ranson Criteria or the APACHE II score to predict clinical outcomes, but measuring the subjective, raw terror of the pain itself remains notoriously difficult. Honestly, it's unclear why certain individuals suffer vastly more intense agony than others with identical laboratory markers. A patient might present with a wildly elevated serum amylase level that is three times the upper limit of normal yet complain of manageable discomfort, while another individual with modest enzyme elevations might be screaming for high-dose intravenous opioids. Experts disagree on whether this discrepancy stems from genetic variations in nerve density or the rapid kinetic speed at which the initial inflammation explodes across the retroperitoneum.
The Atlanta Classification and What It Means for Your Nerves
When analyzing how pancreatitis is one of the most painful conditions, we must look at the 2012 revised Atlanta Classification, which helpfully divides the disease into mild, moderately severe, and severe categories. In the mild form, which thankfully accounts for about 80% of all hospital admissions, the inflammation is interstitial and edematous. It is brutal, yes, but typically resolves within a week. Where it gets tricky is when a patient transitions into necrotizing pancreatitis, a catastrophic variant where parts of the organ actually die due to a complete lack of blood flow. This necrotic tissue frequently becomes infected, triggering a systemic inflammatory response syndrome (SIRS) that sends the entire central nervous system into a state of hyperalgesic shock.
The Hidden Onset Timeline
But the real terror lies in the sheer velocity of the assault. Unlike a slow-burning ulcer or the gradual build-up of a chronic infection, acute pancreatitis peaks with terrifying speed, often reaching maximum, blinding intensity within a mere 10 to 30 minutes of the initial trigger. There is no ramp-up period. One minute you are finishing a heavy dinner at a restaurant, and the next you are in the back of an ambulance clutching your epigastrium in absolute bewilderment.
The Dueling Triggers: Gallstones versus Ethanol Abuse
While the end result is almost always an agonizing stay in a sterile hospital room, the path to getting there usually splits into two primary, distinct clinical avenues. These two etiologies account for roughly 75% of all diagnosed cases worldwide, yet they behave in markedly different ways inside the abdomen.
The Mechanical Violence of Cholelithiasis
Let us look at biliary pancreatitis first, which is primarily driven by gallstones migrating out of the gallbladder. If a stone gets lodged at the Ampulla of Vater—the narrow, shared exit gateway where the common bile duct and the main pancreatic duct meet—it creates an instant, catastrophic pressure backup. I have looked at countless imaging reports from cases in metropolitan centers like Chicago and London, and the mechanical reality is always chilling: the pancreas keeps pumping out fluid against a structural wall, causing intraductal pressure to skyrocket until the microscopic ducts literally rupture from the strain. This sudden, explosive mechanical failure is why biliary cases often present with the most immediate, shocking spikes of acute pain.
The Slow Toxic Burn of Chronic Alcohol Consumption
In stark contrast, alcohol-induced pancreatitis operates via a far more insidious, metabolic mechanism. Chronic ethanol exposure alters the permeability of the pancreatic ductules and increases the protein concentration of pancreatic secretions, leading to the formation of dense protein plugs that slowly choke the organ's drainage system from within. It is a slow, toxic smoldering process. Yet, the issue remains that because alcohol also acts as a central nervous system depressant during initial consumption, many patients ignore the early, warning twinges of pancreatic distress until the organ reaches a definitive, irreversible tipping point of widespread inflammation.
How Pancreatitis Pain Measures Up Against Other Medical Horrors
To truly understand if pancreatitis is one of the most painful events a human can endure, it helps to place it side-by-side with other legendary clinical nightmares. We are talking about conditions that routinely break the standard zero-to-ten pain scale utilized in triage units.
The Agony Hierarchy: Pancreas versus Kidney Stones and Labor
Consider the classic nephrolithiasis, or kidney stone. Anyone who has passed a jagged calcium oxalate crystal through a microscopic ureter will tell you it feels like being stabbed with a rusty file. However, kidney stone pain is famously colicky; it arrives in distinct, rhythmic waves, offering brief, merciful windows of exhaustion between spasms. Pancreatitis offers no such quarter. It is a solid, crushing wall of unremitting torment that does not ebb or flow. When compared to the contractions of active human labor, women who have unfortunately experienced both conditions have explicitly stated that while childbirth has a profound, instinctual biological purpose and natural hormonal pauses, the artificial, toxic burn of an inflamed pancreas feels like an unnatural, existential threat to survival. We are far from a simple stomach ache here; it is an entirely different beast.
Common mistakes and misconceptions about pancreatic inflammation
The myth of the exclusive alcohol trigger
People assume a damaged pancreas equals a history of heavy drinking. This assumption is flawed. While chronic alcohol abuse undeniably wreaks havoc on pancreatic tissues, biliary sludge and rogue gallstones actually trigger up to 40% of acute pancreatitis episodes worldwide. Idiopathic cases—where science simply shrugs its shoulders—account for another frustrating 20%. Let's be clear: assuming someone brought this agonizing torture upon themselves through lifestyle choices is a medical insult. Genetic mutations, hypercalcemia, and even mundane prescription medications can spark the exact same internal wildfire. Why does this stigma persist? Because society loves a simple cause-and-effect narrative, even when biology refuses to cooperate.
Is pancreatitis one of the most painful conditions, or just indigestion?
Dismissing the initial twinges as a simple case of acid reflux or a temporary stomach bug is a dangerously frequent blunder. The pancreas sits deep within the retroperitoneal space. This anatomical positioning means early swelling mimics standard gastric distress, leading patients to pop antacids while their internal organs literally digest themselves. By the time the realization hits that this is no ordinary bellyache, the inflammatory cascade is already out of control. Waiting out the storm at home frequently results in hypovolemic shock. Do not mistake a catastrophic organ failure for a bad burrito.
The misconception of the quick fix
Surviving the initial, excruciating hospitalization gives patients a false sense of total victory. They believe a few days of intravenous fluids and bowel rest cures the ailment completely. Except that the pancreas possesses a notoriously long memory. Microscopic scarring alters enzyme secretion permanently in many individuals. Post-pancreatitis exocrine insufficiency plagues roughly one-third of patients post-discharge, requiring lifelong enzyme replacement therapy. A singular acute attack can quietly transition into a simmering, lifelong battle against chronic tissue degradation.
The microvascular nightmare and expert management advice
The hidden ischemic breakdown
We focus heavily on the crushing neural signals, but the true villain behind the longevity of this agony is microvascular failure. When the pancreas inflames, local capillaries constrict violently and then become pathologically permeable. Is pancreatitis one of the most painful experiences known to medicine? Yes, precisely because this vascular collapse starves the surrounding tissue of oxygen, inducing localized necrosis. It is a ischemic crisis disguised as a digestive problem. Doctors must aggressively manage fluid resuscitation within the first 24 hours of symptom onset to keep these tiny vessels open. If you miss this therapeutic window, tissue death accelerates exponentially.
Advocating for aggressive, multi-modal analgesia
Standard over-the-counter pain relievers are utterly useless here. Experts now advocate for early, aggressive utilization of patient-controlled analgesia (PCA) pumps, frequently employing synthetic opioids like fentanyl alongside adjuvant regional nerve blocks. The issue remains that traditional medical training instilled a lingering fear of inducing sphincter of Oddi spasms with certain narcotics (a theoretical worry that modern clinical trials have largely debunked). Waiting for pain to peak before administering the next dose is a systemic failure. We must get ahead of the neurological pain pathways before spinal cord sensitization locks the patient into a state of hyperalgesia.
Frequently Asked Questions
How long does the peak agony of an acute attack typically last?
The unrelenting, stabbing pain of a severe acute episode generally commands its maximum intensity for 48 to 72 hours after the initial onset. During this critical window, serum amylase and lipase levels frequently skyrocket to more than three times the upper limit of normal range. Patients require continuous intravenous narcotic infusions to make this window remotely bearable. But can the discomfort linger beyond this timeframe? Absolutely, as localized fluid collections and pseudocysts can prolong the mechanical pressure on surrounding nerve plexuses for several weeks, requiring prolonged hospitalization in up to 25% of severe cases.
Can a specific diet completely prevent a future pancreatitis relapse?
No dietary regime offers an absolute, ironclad guarantee against recurrence, though strict mitigation strategies drastically alter your statistical odds. Patients must rigidly restrict their daily fat consumption to less than 30 grams per day to minimize the stimulation of pancreatic digestive enzymes. Avoiding alcohol entirely is mandatory, regardless of the original etiology of your specific attack. Yet, if your underlying trigger is an untamed genetic mutation or an anatomical anomaly like pancreas divisum, even the most pristine, fat-free lifestyle cannot fully neutralize the inherent biological risk of another flare-up.
Why does the pain frequently radiate directly into the patient's back?
The peculiar, boring sensation that travels directly through to the spine is due to the retroperitoneal location of the pancreas. It rests immediately anterior to the celiac plexus, a massive, dense network of interconnected nerves. As the organ swells and autodigestion commences, inflammatory cytokines directly bathe these sensitive nerve fibers. This anatomical proximity explains why sitting upright or leaning forward slightly alleviates the pressure, whereas lying flat on your back forces the heavy, inflamed organ directly onto the neural bundle, magnifying the torment. (Most patients instinctively curl into a fetal position on the hospital gurney to find a shred of comfort.)
The reality of pancreatic torment
We must stop treating pancreatitis as just another item on the long list of gastrointestinal complaints. It belongs in the absolute highest tier of human physical suffering, right alongside active myocardial infarctions and advanced bone cancer metastases. Medical protocols must evolve to reflect this terrifying reality through faster triage times and immediate, mandatory access to high-tier regional anesthesia. To minimize this condition as mere abdominal discomfort is a failure of empathy and clinical judgment. As a result: we need a radical shift toward aggressive, early intervention strategies that prioritize neurological dampening alongside fluid resuscitation. Let us be utterly uncompromising in how we validate and treat this anatomical catastrophe.