The Anatomy of a Hidden Time Bomb: What We Get Wrong About Vascular Weakness
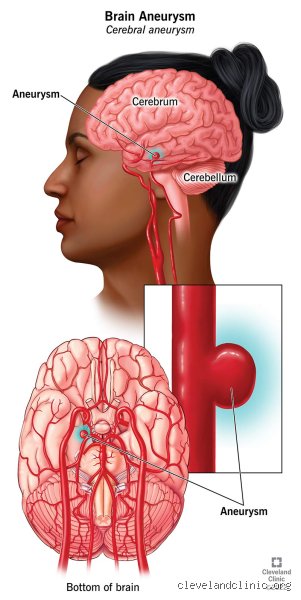
We like to imagine our arteries as reinforced steel pipes, but they are actually closer to high-pressure garden hoses made of living tissue that can, under the right (or wrong) circumstances, develop a structural flaw. An aneurysm is essentially a pathological bulge in the wall of a blood vessel, usually occurring at branching points where the turbulence of blood flow is at its most chaotic. Think of it like a weak spot on a tire that begins to bubble outward; as long as the rubber holds, you drive on unaware. People don't think about this enough, but roughly 1 in 50 people in the United States are walking around with an unruptured intracranial aneurysm right now, according to data from the Brain Aneurysm Foundation. Most of these individuals will live their entire lives, die of old age, and never realize their biology had a secret.
The Hemodynamic Stress Test
Why do some vessels hold while others fail? It comes down to the tunica media, the muscular middle layer of the artery that provides its elasticity and strength. In an aneurysm, this layer thins out or disappears entirely, leaving only the fragile inner and outer membranes to hold back the pulsing tide of systolic pressure. But here is where experts disagree: we still cannot perfectly predict which 5mm bulge will stay dormant for decades and which will suddenly give way during a morning jog. I believe the medical community relies too heavily on size as the sole predictor of risk, often overlooking the morphological irregularity of the sac itself. A small, "nubbly" aneurysm might actually be more dangerous than a larger, smooth one. Which explains why some patients are told to "watch and wait" while others are rushed into the catheterization lab for immediate coiling.
Can You Actually Miss the Moment of Rupture?
The idea that you could sleep through a ruptured brain aneurysm is, honestly, a bit of a medical fairy tale, yet the nuances of "sentinel bleeds" complicate the narrative. When a subarachnoid hemorrhage occurs, blood escapes the high-pressure arterial system and sprays into the space surrounding the brain, instantly increasing intracranial pressure. This isn't a dull ache. It is often described as a "thunderclap headache," reaching peak intensity within 60 seconds. But—and this is a massive caveat—about 15% to 60% of patients experience what doctors call a warning leak days or weeks before the big event. These minor ruptures involve a tiny amount of blood that the body quickly manages, resulting in a headache that might feel "different" but not necessarily "deadly." That changes everything for the diagnostic process. If you dismiss that strange, sharp pain as a result of stress or a neck strain, you might technically "not know" you've had a minor rupture, even though your body screamed the news at you.
The Aortic Exception and the Fog of Pain
The issue remains even more obscured when we talk about the aorta, the body’s massive main highway. An Abdominal Aortic Aneurysm (AAA) can grow to the size of a grapefruit without causing a single symptom. If it ruptures, the sensation is usually a sudden, tearing pain in the back or abdomen, often accompanied by a rapid drop in blood pressure that leads to fainting. Could you miss it? Only if you lose consciousness so fast that your brain doesn't have time to process the agony. In the case of a dissection—where the layers of the artery wall tear and blood enters between them—the pain is so distinct that patients in the ER often use the word "ripping" to describe it. We're far from it being a subtle event; it is a systemic collapse. Yet, if the patient is elderly or has advanced neuropathy from diabetes, the sensory feedback might be slightly dulled, leading to a delay in seeking help that proves fatal.
Technical Mechanics of the Vascular Breakdown
To understand the "silent" aspect, we have to look at the transmural pressure across the vessel wall. As the diameter of the aneurysm increases, the tension on the wall grows exponentially—a physical law known as Laplace’s Law ($T = \frac{Pr}{w}$). As a result: the thinner the wall gets, the more stress it bears, creating a vicious cycle of expansion. At the moment of rupture, the sheer force of the blood exiting the vessel causes a vasospasm, where neighboring arteries constrict in a desperate, often counterproductive attempt to stop the bleeding. This vasospasm can cause secondary strokes, which further muddies the clinical picture. A patient might wake up with a numb arm and think they slept on it funny, not realizing that a tiny bleed hours earlier has triggered a cascade of neurological failures. Because the brain itself doesn't have pain receptors, the "headache" actually comes from the irritation of the meninges, the sensitive linings around the brain. If the bleed is small enough and tucked away, the irritation might be localized, leading to a misdiagnosis of a "crick in the neck."
The Genetic and Environmental Synergy
It is not just bad luck; it's a biochemical conspiracy involving your DNA and your lifestyle choices. Specifically, certain connective tissue disorders like Ehlers-Danlos syndrome or Polycystic Kidney Disease (PKD) significantly weaken the arterial walls from birth. Add chronic hypertension into the mix—which keeps the "pipe" under constant overpressure—and you have the perfect recipe for a blowout. Interestingly, researchers at the Mayo Clinic have noted that smoking is perhaps the single greatest modifiable risk factor, as it introduces toxins that actively degrade the structural proteins within the vessel walls. Yet, we see cases every year of marathon runners in their 30s collapsing from a ruptured Berry Aneurysm. It’s a sobering reminder that while we can manage the odds, we cannot eliminate the inherent fragility of being a pressurized biological system. The issue remains that we often don't screen for these unless a family history exists, which seems like a massive oversight in preventative medicine.
Comparing the "Worst Headache" to Routine Migraines
How do we distinguish between a life-threatening emergency and a routine, albeit painful, migraine? The distinction lies in the temporal profile of the pain. A migraine usually ramps up over an hour, often preceded by an aura or light sensitivity, whereas a rupture is binary—one second you are fine, and the next you are on the floor. However, the nuance comes with thrombosed aneurysms, where a blood clot forms inside the bulge. This can cause a dull, steady aching as the clot pushes against surrounding nerves (like the third cranial nerve, leading to a drooping eyelid). In this specific scenario, you might have a "leaking" or "growing" aneurysm that you misinterpret for weeks. Statistics show that roughly 25% of patients with a subarachnoid hemorrhage are initially misdiagnosed because their symptoms weren't "textbook" enough. We must stop assuming that every rupture looks like a Hollywood heart attack. Sometimes, it looks like a middle-aged woman sitting in a darkened room with a damp cloth on her forehead, wondering why her usual aspirin isn't working.
The Role of Silent Ischemia
In rare instances, an aneurysm doesn't rupture so much as it "erodes." If an aneurysm in the carotid artery presses against a nerve or sheds tiny clots—a process called microembolization—the patient might experience "silent" mini-strokes or Transient Ischemic Attacks (TIAs). These are technically complications of an aneurysm that you could easily ignore. A brief moment of blurred vision? You blame your contact lenses. A temporary tingle in your fingers? You blame your keyboard ergonomics. But these are the subtle breadcrumbs leading to a catastrophic rupture. The issue remains that our bodies are masters of compensation, masking minor failures until the system can no longer bridge the gap. In short, while you won't miss the final explosion, you are almost certainly missing the dozens of tiny "pings" the system sends out as it approaches the breaking point. The transition from unruptured to ruptured is a cliff, not a slope.
Common misconceptions and the "sentinel" fallacy
The problem is that most people envision a vascular catastrophe as a cinematic explosion. They expect a thunderous clap of agony that instantly grounds the victim, but biology rarely follows a Hollywood script. Silent seepage, often clinically termed a sentinel bleed, occurs in up to 30 percent of subarachnoid hemorrhages. You might experience a nagging "warning headache" that mimics a common migraine or a tension-related episode. Because these precursors are often transient, patients ignore them. But we must be honest: ignoring a sudden, localized pressure change in your cranium is a gamble with your neurological future. Let's be clear, a minor leak is still a rupture. It just has not reached its final, devastating velocity yet.
The "size equals safety" myth
Many patients assume that a small protrusion, perhaps under 5 millimeters, is incapable of structural failure. Except that hemodynamic stress does not care about your arbitrary thresholds. While the PHASES score provides a statistical framework for risk, it is not a prophetic crystal ball. Data suggests that approximately 10 to 15 percent of ruptured aneurysms were smaller than the standard 7-millimeter intervention threshold. Wall tension and localized inflammation can cause a tiny sac to fail while a larger, calcified one remains stable for decades. Thinking you are safe just because a scan showed a "small" lesion is a dangerous psychological comfort that ignores the fluid dynamics of high blood pressure.
The confusion with chronic sinus issues
The issue remains that the location of a bulging vessel often mimics less severe pathologies. A posterior communicating artery aneurysm can press against the oculomotor nerve, causing a drooping eyelid or double vision. Do you know how many people mistake this for an allergy flare-up or simple fatigue? (Spoiler: too many). By the time the patient realizes their "sinus pressure" is actually a hemodynamic structural failure, the window for preventative coiling or clipping has slammed shut. It is an irony of the human body that our most critical alarms often sound identical to a seasonal cold.
The hemodynamic invisible: Expert advice on screening
If you are walking around wondering can an aneurysm rupture without you knowing, you need to look at your genetic blueprint rather than just your symptoms. Professional consensus is shifting toward more aggressive screening for those with two or more first-degree relatives affected by intracranial berry aneurysms. Smoking remains the single most modifiable risk factor, as it increases the rate of growth by nearly four times compared to non-smokers. Which explains why clinicians are increasingly stubborn about nicotine cessation in vascular patients. It is not just about lung health; it is about keeping the collagen in your arterial walls from degrading into a state of irreparable fragility.
The role of MRA and CTA imaging
As a result: we rely on Magnetic Resonance Angiography to spot these hidden threats before they declare themselves through a bleed. A standard MRI might miss the specific vascular architecture, so asking for a dedicated "vessel study" is paramount if you have a family history. Experts now emphasize that asymptomatic detection is the only way to truly "know" before the wall gives way. We have limits, of course. We cannot scan every person with a headache. However, for those in high-risk categories, the cost of an elective scan is negligible compared to the 40 percent mortality rate associated with an initial subarachnoid event. Awareness is your only shield against a process that is essentially a structural engineering failure inside your head.
Frequently Asked Questions
Can you survive a ruptured aneurysm for days without medical treatment?
It is statistically rare but biologically possible for a patient to survive several days with a low-grade subarachnoid hemorrhage. Data indicates that about 15 to 20 percent of patients may experience a "warning leak" where the bleeding is contained enough to avoid immediate coma. These individuals often complain of a persistent, stiff neck and a sensitivity to light that does not resolve with standard painkillers. However, the risk of a massive secondary re-rupture within the first 24 to 48 hours is approximately 20 percent, making delayed treatment a lethal decision. Without intervention, the blood eventually clogs the drainage pathways of the brain, leading to hydrocephalus or a final, fatal stroke.
Does a rupture always cause a loss of consciousness?
No, a significant portion of patients remain awake and alert during the initial stages of a vascular breach. While the classic "thunderclap headache" is present in nearly 95 percent of cases, a loss of consciousness only occurs in about half of those patients. You might simply feel a sudden, agonizing jolt that fades into a dull ache, leading you to believe the "worst" has passed. This is a cognitive trap because vasospasm, a delayed narrowing of the arteries due to blood exposure, typically peaks between days 3 and 14 after the event. Even if you stay awake, the chemical environment of your brain is rapidly deteriorating after the first drop of blood escapes.
How often are these events completely "silent" in medical imaging?
Modern CT scans are incredibly sensitive, catching roughly 98 percent of subarachnoid hemorrhages if performed within the first six hours of symptom onset. After 24 hours, the sensitivity of a standard CT drops to about 90 percent as the body begins to process and clear the extravasated blood. For patients who wait several days to seek help, a lumbar puncture may be required to look for xanthochromia, which is a yellow discoloration of the spinal fluid. This diagnostic tool can detect blood breakdown products for up to two weeks after a suspected rupture. In short, while the event might feel silent to the patient, it leaves a chemical trail that medical science can almost always identify if the right tests are ordered.
The verdict on vascular vigilance
The medical community must stop treating the question of can an aneurysm rupture without you knowing as a simple yes or no binary. We have spent decades obsessed with the "explosion" while ignoring the micro-bleeds and nerve compressions that serve as the body's final frantic telegrams. Let's take a stand: the current reactive model of waiting for a catastrophe is an archaic failure of preventative medicine. You cannot feel your blood pressure, and you cannot feel the thinning of an arterial wall until it is nearly too late. Waiting for the "worst headache of your life" is not a health strategy; it is a neurological Russian roulette. We need to prioritize elective screening for at-risk populations and stop dismissing atypical headaches as mere stress. Your brain is a high-pressure system, and in the world of vascular integrity, unearned confidence is the most dangerous symptom of all.