The Ticking Clock Inside the Skull: What We Are Actually Dealing With
Let us strip away the sterile clinical language for a moment. An unruptured brain aneurysm is essentially a blister on a blood vessel, a structural weakness where the muscular wall of an artery gives way under the relentless thumping of cardiac pressure. Statistics from the Brain Aneurysm Foundation indicate that roughly 1 in 50 people in the United States harbor one of these intracranial anomalies right now. Most individuals will live their entire lives oblivious to the ticking clock inside their heads, dying of something else entirely. But when a bubble expands to 7 millimeters or larger—the threshold where neurosurgeons at institutions like the Mayo Clinic start sweating—the physics of the skull change.
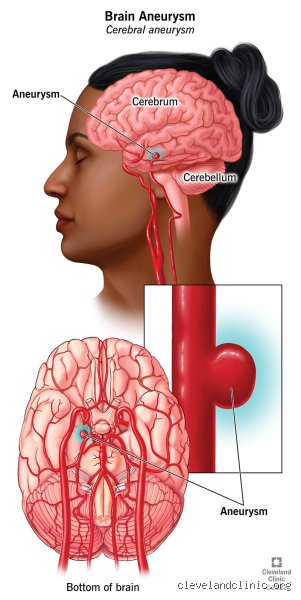
The Anatomy of a Cerebral Bulge
Why do these arterial outpouchings form in the first place? It is a cocktail of genetic bad luck, chronic hypertension, and the shearing stress of turbulent blood flow, particularly at the bifurcations of the Circle of Willis. This vascular ring sits at the base of the brain, routing blood to the anterior, middle, and posterior cerebral arteries. When the internal elastic lamina degrades, the pressure pushes the vessel wall outward, creating a saccular, or berry, aneurysm. Fusiform aneurysms, which dilate the entire circumference of the artery, are rarer but equally problematic. Yet, the brain parenchyma itself lacks pain receptors.
Where the Pain Logic Fails
Because the brain tissue cannot feel pain, traditional teaching dictated that an unruptured brain aneurysm could not hurt. I find this clinical dogma dangerously reductive. Surrounding these vessels are pain-sensitive structures: the meninges, large cranial nerves, and the dura mater. When an aneurysm expands, it does not exist in a vacuum. It crowds its neighbors. If a bulge presses against the ophthalmic branch of the trigeminal nerve, you are going to feel it, regardless of what the textbook says.
The Mechanics of Pain: How an Intact Aneurysm Signals Distress
Where it gets tricky is differentiating between a standard tension headache and a warning sign from a ballooning vessel. When an unruptured brain aneurysm does cause discomfort, it is rarely a diffuse, dull ache. Instead, it presents as a localized, boring pain, often described by patients as a hot poker behind one eye or a relentless pressure in a specific quadrant of the skull. This is not the agonizing, explosive thunderclap headache associated with a subarachnoid hemorrhage—that changes everything, turning a medical watch-and-wait scenario into an immediate fight for survival. Instead, this is a slow-burn herald symptom.
Mass Effect and Nerve Compression
The primary mechanism for pain in non-ruptured cases is the mass effect. Think of it like a tumor, except this tumor expands and contracts with every single heartbeat. A classic example involves an aneurysm located at the junction of the internal carotid artery and the posterior communicating artery. As it grows, it directly compresses the third cranial nerve, also known as the oculomotor nerve. The result? A dull, deep ache behind the orbit, accompanied by a drooping eyelid—ptosis—and a dilated pupil that refuses to react to light. In 2022, researchers at Johns Hopkins documented that over 35 percent of patients with large posterior communicating artery aneurysms experienced localized orbital pain before any surgical intervention.
Micro-Leaks and Wall Inflammation
But what about smaller bulges that do not touch a nerve? This is where the issue remains highly debated among top-tier endovascular specialists. Some studies suggest that the pain arises from microscopic tracking of blood into the vessel wall itself, a process known as dissection, or from localized macrophage infiltration that triggers an inflammatory cascade in the adventitia. The vessel wall becomes inflamed. It stretches. It hurts. And because the perivascular nerve plexus is rich with nociceptive fibers, your body registers the structural failure long before the dam actually breaks.
Deciphering the Symptoms: Is It a Migraine or Something Worse?
We live in a world where millions suffer from chronic migraines, making the diagnosis of an unruptured brain aneurysm incredibly messy. How does a clinician in an emergency room in Chicago or London separate a routine neurological event from a vascular emergency? Honestly, it's unclear without advanced neuroimaging like a Computed Tomography Angiography or a Magnetic Resonance Angiography. But patients know their bodies, and an aneurysm headache usually lacks the classic migraine aura, nausea, or sensitivity to light. It is architectural pain, not electrical dysfunction.
The Localized Sentinel Headache
The medical community uses the term sentinel headache to describe a warning pain that precedes a major rupture. While historically attributed to minor blood leaks, contemporary tracking shows these headaches can be purely mechanical. In a landmark 2019 retrospective study published in the Journal of Neurosurgery, analysts looked at 412 patients diagnosed with unruptured brain aneurysms. A striking 18.4 percent of them presented with isolated headaches as their primary complaint, with no evidence of subarachnoid blood on high-resolution imaging. People don't think about this enough: a headache can be a structural warning, not just a chemical imbalance.
Comparing Diagnostic Trajectories: Routine Screenings Versus Symptomatic Discoveries
The way we discover these vascular vulnerabilities radically alters the psychological and physical outcome for the patient. The vast majority of unruptured brain aneurysms are found entirely by accident—incidentalomas, as radiologists like to call them. You trip on a curb, hit your head, get an MRI to rule out a concussion, and suddenly you are looking at a 4-millimeter bubble on your middle cerebral artery. This is a far cry from the patient who arrives at the clinic demanding answers for an unyielding, focal pain that has resisted every triptan and NSAID on the market.
The Incidental Discovery Conundrum
When an aneurysm is found incidentally, the clinical path is often conservative management, especially if it is small and located in the anterior circulation. The annual rupture rate for a 3-millimeter anterior aneurysm is less than 0.1 percent, according to data from the International Study of Unruptured Intracranial Aneurysms. Doctors look at those odds and decide the risks of brain surgery outweigh the risks of leaving it alone. Yet, for the symptomatic patient, those statistical models are essentially useless. If an unruptured brain aneurysm hurts, the structural integrity of the vessel is already compromised, or it is growing rapidly, which flips the risk-benefit analysis entirely on its head.
Common mistakes and dangerous misconceptions
The "silent until it pops" myth
We need to discard the outdated notion that unruptured brain aneurysms hurt absolutely nothing until a catastrophic hemorrhage occurs. This black-and-white thinking dominates online forums. The problem is, biology rarely respects our neat binaries. While up to 90 percent of these vascular anomalies remain entirely asymptomatic throughout a patient's lifetime, the remaining subset actively signals trouble. Dismissing atypical localized facial pain or a sluggish pupil simply because "unruptured lesions are silent" represents a hazardous clinical oversight. Let's be clear: a structural defect ballooning inside your cranium can exert mechanical pressure long before the tissue fails.
Confusing standard migraines with sentinel headaches
Do unruptured brain aneurysms hurt in the exact same manner as a bad hangover or a routine stress episode? Not quite. Yet, millions of individuals misinterpret localized, Boring-type cranial pain as a simple migraine variant. This diagnostic confusion delays life-saving imaging. Standard migraines typically feature throbbing, widespread discomfort accompanied by severe light sensitivity, whereas aneurysm-induced pain often manifests as a rigid, localized structural ache behind a single eye. If your standard headache prescription suddenly fails to touch a specific, deep-seated pain point, you are not just having a bad day. You might be experiencing the physical expansion of a vulnerable arterial wall.
The micro-leak phenomenon: Expert insights
Warning shots from the vascular wall
Neurologists are increasingly investigating the concept of "sentinel leaks," which are microscopic trickles of blood that fail to cause a full-blown subarachnoid hemorrhage but irritate neighboring structures intensely. Because the brain tissue itself lacks pain receptors, this specific agony stems directly from the stretching of the heavily innervated arterial wall or meningeal irritation. It is a terrifyingly subtle process. As a result: an individual might experience a sudden, uncharacteristic headache that subsides after forty-eight hours, mistakenly believing the danger has passed. Except that this temporary agonizing spike often represents the final structural warning before a major rupture.
How do we differentiate this from everyday stress? True sentinel pain possesses an explosive, peak-intensity onset that differentiates it from muscle tension. Medical professionals utilize high-resolution magnetic resonance angiograms to detect these structural shifts, recognizing that a changing pain profile often correlates with a 50 percent increase in immediate rupture risk. (Neurosurgeons rarely gamble with changing pain profiles for this exact reason). We cannot afford to treat localized cranial changes with wait-and-see apathy.
Frequently Asked Questions
Can a 3mm unruptured brain aneurysm cause chronic daily headaches?
Statistically speaking, an isolated 3mm lesion lacks the physical mass to compress cranial nerves or trigger ongoing daily discomfort. Large-scale clinical registries indicate that lesions under 5 millimeters possess an annual rupture risk of virtually zero percent in the absence of specific family histories or smoking habits. The issue remains that patients discovering these tiny vascular anomalies via unrelated MRI scans frequently project their preexisting tension headache anxiety onto the incidental finding. In short, while the localized ache is undeniably real to the sufferer, the tiny arterial bulge itself is almost certainly an innocent bystander rather than the root anatomical cause of chronic daily pain.
What does the pain from an expanding unruptured brain aneurysm feel like?
When an unruptured brain aneurysm hurts due to active expansion, the sensation typically mimics a sharp, boring implement driving directly into the orbit of the eye or the temple region. This acute discomfort frequently presents alongside localized neurological deficits, such as a suddenly drooping eyelid or unexplained double vision caused by compression of the adjacent third cranial nerve. Up to 15 percent of patients tracking expanding lesions report these specific focal warning signs prior to definitive surgical intervention. It is a deep, structural distress signal that refuses to fluctuate with neck movement, physical posture, or standard over-the-counter anti-inflammatory medications.
Does stress make an unruptured brain aneurysm hurt more?
Psychological stress does not directly inject pain into the lesion itself, but acute emotional upheaval dramatically spikes your systemic blood pressure. Which explains why sudden hypertensive surges can cause a vulnerable, thinning arterial wall to stretch further and trigger localized discomfort. Clinical data demonstrates that acute systolic blood pressure spikes exceeding 160 mmHg significantly increase transmural pressure across the aneurysm wall. This mechanical strain can induce a sudden dull ache in a previously silent lesion, serving as a physical manifestation of vascular stress. Therefore, managing emotional turbulence is not merely a lifestyle recommendation; it is a direct method of stabilizing intracranial physics.
A definitive stance on cranial pain and vascular anomalies
Medical conservatism loves to tell patients that their head pain is unrelated to their newly discovered vascular bulges. We must challenge this blanket dismissiveness because treating every unruptured brain aneurysm as a silent, benign spectator ignores the nuanced realities of intracranial pressure dynamics. When an unruptured brain aneurysm hurts, it represents a breakdown in structural equilibrium that demands immediate, objective investigation rather than diagnostic gaslighting. We cannot accurately predict which specific headache precedes a catastrophic neurological event based on reassurance alone. Ultimately, erasing the dogma surrounding these lesions is the only way to prevent avoidable tragedies before the pressure becomes too great.