The PDA Puzzle: Why It’s Overlooked in Girls
Autism diagnoses have historically favored male presentations—we’re talking repetitive behaviors, rigid routines, obvious social disconnect. But for females, especially those with Pathological Demand Avoidance, the signs are subtler. They mimic shyness, anxiety, or even oppositional behavior. A girl might agree to do her homework, then vanish into a book, claiming she was “just finishing a chapter.” Is she stalling? Maybe. But in PDA, that’s a real-time negotiation with internal overwhelm. The demand—“do your homework”—triggers a fight-or-flight response, not laziness. And that’s where misunderstanding begins.
Research shows autism is diagnosed in males at a ratio of about 3:1. But when you filter for PDA, the gender gap shrinks. Some clinicians suspect we're missing thousands of girls because their PDA presents as social mimicry, intense emotional reactions, or passive resistance rather than outbursts. They’re not avoiding tasks to be difficult. They’re protecting their nervous systems. Yet, without recognition, they get labeled difficult, anxious, or lazy.
And here’s the kicker: many women with PDA aren’t identified until adulthood—sometimes after their own child receives a diagnosis. That changes everything. You start re-reading your childhood: the meltdowns over getting dressed, the inability to follow simple routines, the way you’d negotiate with teachers to avoid presentations. It wasn’t immaturity. It was neurological.
Defining PDA: Beyond Simple Refusal
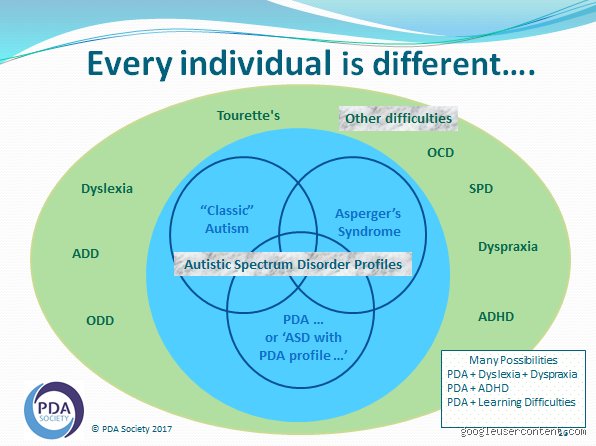
Pathological Demand Avoidance isn’t a standalone diagnosis in manuals like the DSM-5 or ICD-11. Instead, it’s considered a profile of autism spectrum disorder, first described by Elizabeth Newson in the 1980s. The core trait? An anxiety-based need to be in control of one’s environment to avoid the psychological threat of demands—even trivial ones like “good morning” or “would you like a drink?”
What makes PDA different from typical autism or ODD (Oppositional Defiant Disorder)? It’s the role of social manipulation. A child with PDA might use charm, distraction, or humor to deflect a demand. “I can’t brush my teeth right now—I’m saving the world from dragons!” That’s not lying. It’s an improvised escape from anxiety. The brain perceives compliance as loss of autonomy, and the response is immediate and intense.
Gender Differences in PDA Expression
Boys with PDA often display more overt resistance—tantrums, physical refusal, yelling. Girls? They internalize. They smile while shutting down. They agree to things they have zero intention of doing. This masking—what psychologists call “camouflaging”—lets them slip through diagnostic cracks. A 2018 study from the University of Bath found that females with autism are more likely to imitate social behaviors, make eye contact (even when uncomfortable), and suppress stimming, all to blend in.
But that effort is exhausting. And for those with PDA, the pressure of “acting normal” amplifies demand avoidance. You can’t comply with social demands if your brain interprets them as threats. So girls might develop elaborate scripts, avoid eye contact through hair-flicking, or retreat into fantasy worlds. They’re not disengaged. They’re surviving.
How PDA Manifests in Daily Life: From Morning Routines to Social Norms
Mornings are minefields. Getting dressed, brushing teeth, eating breakfast—each step is a demand. For a girl with PDA, this isn’t procrastination. It’s a neurological blockade. The brain says: “This is not safe.” And the body responds with paralysis, meltdowns, or distraction tactics. You’ve probably seen it: the child suddenly becoming fascinated by a dust speck on the wall when asked to put on shoes. That’s not defiance. That’s self-regulation.
School environments are especially tough. Rigid schedules, teacher instructions, group work—all constant demands. A girl might appear cooperative in class but collapse at home. Or she might use social intelligence to negotiate her way out: “Can I do that tomorrow? I’ll write an extra paragraph.” This works—until it doesn’t. Teachers see inconsistency. Parents see laziness. The child sees only survival.
And what about social interactions? Invitations, greetings, even small talk count as demands. A simple “how are you?” can trigger anxiety. The expected response—“I’m fine”—feels like a trap. What if she’s not fine? What if she says too much? So she avoids. Or deflects. Or gives a scripted answer. The problem is, others don’t see the internal calculus. They see rudeness.
Because PDA is rooted in anxiety, not opposition, punishment rarely works. In fact, it backfires. The more pressure applied, the stronger the resistance. It’s a paradox: trying to force compliance increases the very behavior you want to reduce.
Why Traditional Discipline Fails with PDA
You can’t “toughen up” someone out of PDA. Threats, rewards, time-outs—they add pressure. Imagine being told to relax while standing on a ledge. That’s the PDA experience. Demands increase anxiety, anxiety increases avoidance, and avoidance gets punished. It’s a cycle that erodes self-worth.
Effective strategies? Reduce direct demands. Use indirect language. Instead of “put on your coat,” try “I’m putting on my coat—brr, it’s cold out.” Offer choices: “Do you want to leave in five minutes or ten?” Use play and imagination: “The coat monster needs feeding—can you help?” It sounds silly. But for a child with PDA, it removes the threat of control.
The Role of Anxiety and Control in PDA Behavior
Anxiety isn’t a side effect of PDA—it’s the engine. Every demand, no matter how small, is assessed for threat level. A request to “say goodnight” isn’t just words. It’s a loss of autonomy, a reminder of expectation. The brain’s amygdala lights up. Fight, flight, freeze, or fawn—those are the options.
That’s why control is non-negotiable. Not control over others, but over one’s own actions. A girl with PDA isn’t trying to dominate a household. She’s trying to prevent psychological overload. And when control is taken away—through force, guilt, or pressure—meltdowns follow. These aren’t tantrums. They’re nervous system explosions.
PDA vs. Other Conditions: Untangling the Confusion
PDA gets mistaken for a lot of things. Oppositional Defiant Disorder? ADHD? Anxiety disorders? All possible misdiagnoses. But the core difference lies in motivation. ODD involves anger and defiance. ADHD involves impulsivity and inattention. PDA? It’s about anxiety-driven avoidance of perceived demands—even desired ones.
Take homework. A child with ADHD might forget or get distracted. A child with ODD might refuse out of anger. A child with PDA? She might want to do the homework but be paralyzed by the demand itself. The thought of starting triggers anxiety, not rebellion. It’s a critical distinction.
PDA vs. ODD: Same Behavior, Different Roots
Both might involve refusal, negotiation, or meltdowns. But ODD is emotionally driven—resentment, irritation, defiance. PDA is anxiety-driven. The child isn’t angry at the parent; she’s terrified of losing control. Punishment worsens ODD. It destroys PDA coping mechanisms.
PDA and ADHD: Overlapping Symptoms, Different Mechanisms
Impulsivity, distractibility, social challenges—ADHD and PDA share traits. But ADHD’s core is executive dysfunction. PDA’s core is demand avoidance due to anxiety. A child with ADHD might start five tasks and finish none. A child with PDA might avoid starting any task because the act of beginning feels threatening.
Frequently Asked Questions
Can PDA Be Diagnosed in Adults?
Yes, though it’s rare. Most adult diagnoses happen retroactively, often after a child’s diagnosis. Self-identification is common. But formal recognition? That’s trickier. Since PDA isn’t in standard diagnostic manuals, clinicians rely on autism assessments with PDA-informed frameworks. The process can take months, involve interviews, and cost anywhere from $1,200 to $3,000 in private settings—insurance coverage varies.
Is PDA More Common in Females Than We Think?
We’re far from it in terms of accurate data. Current prevalence estimates suggest PDA may affect 1 in 20 autistic individuals, but gender-specific stats are scarce. Clinicians like Judith Gould argue that because girls mask better, PDA in females is undercounted. It’s not that PDA is rarer in girls—it’s that it’s harder to see.
What Support Strategies Work Best for Girls with PDA?
Reduce direct demands. Use collaboration, not control. Offer choices. Leverage interests. A girl obsessed with horses might write a story about a horse doing math instead of doing math herself. Humor helps. So does flexibility. But here’s my take: stop pathologizing avoidance. Start seeing it as communication. If a child refuses, ask: what’s the demand? What’s the fear? And why does she feel unsafe complying?
The Bottom Line: Recognizing PDA Is an Act of Empathy
Let’s be clear about this: PDA in females isn’t a discipline problem. It’s a neurological reality masked by gender expectations. We expect girls to be compliant, quiet, accommodating. When they’re not, we blame personality, not neurology. That needs to change. I find this overrated idea—that willpower can overcome anything—especially damaging for PDA. You can’t “try harder” your way out of a brain that interprets “pass the salt” as a threat.
The answer isn’t more structure. It’s more understanding. More flexibility. More willingness to see behind the behavior. Data is still lacking, experts disagree on diagnostic criteria, and honestly, it is unclear how many women live undiagnosed. But one thing’s certain: when we stop seeing avoidance as defiance and start seeing it as protection, we open doors. And that changes everything. (Even if progress is slow—like 0.3% of autism research funding focused on PDA slow.)