The Truth Behind the Geriatric Pregnancy Myth and Why We Need a New Timeline
The medical establishment loves a rigid boundary. For decades, the turning of a thirty-fifth birthday automatically stamped a woman’s prenatal chart with the ominous term geriatric pregnancy—a linguistic relic that honestly belongs in a Victorian museum. Why this specific number? The origin story of the advanced maternal age designation tracks back to the late 1970s when amniocentesis technology first gained traction. Doctors calculated that the risk of miscarriage from the procedure itself roughly balanced the statistical risk of chromosomal abnormalities at age 35, establishing an arbitrary line in the sand. But society changed; the science did not immediately catch up. We live in an era where the average age of first-time mothers in metropolitan hubs like New York, London, and Tokyo has soared, yet our psychological framing remains trapped in the twentieth century. The thing is, your ovaries do not self-destruct at midnight on your 35th birthday. It is a slope, not a cliff.
The Statistical Distortion of Fertility Data
Much of the terrifying data thrown at women today relies on historical records that predated modern antibiotics, let alone IVF. Did you know a frequently cited statistic about female infertility comes from French birth registries spanning the years 1670 to 1730? Relying on centuries-old data to plan a family in the modern world seems absurd, doesn't it? When a 2004 study by psychologist David Dunson examined modern women, researchers discovered that 82 percent of women aged 35 to 39 conceived within a year of regular unprotected intercourse. That changes everything. Compare that to the 86 percent success rate of women aged 27 to 34, and the terrifying drop-off starts to look much more like a gentle slope.
The Biological Ledger: Oocyte Quality vs. Quantity After 35
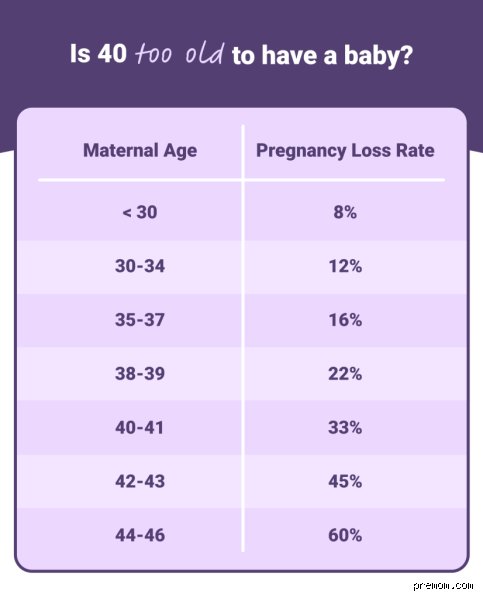
Where it gets tricky is the inescapable reality of ovarian reserve. Every woman is born with her lifetime supply of eggs—roughly one to two million oocytes waiting in the wings since embryonic development. By puberty, that number drops to about 300,000, and from that point onward, the body discards thousands of eggs every single month regardless of whether you are on birth control, pregnant, or abstinent. By the time you hit 35, the remaining pool hovers around 25,000 to 30,000. Quantity matters, yet quality dictates the game. As oocytes age within the ovaries, they become more prone to errors during the delicate process of cellular division known as meiosis. This specific cellular instability frequently leads to aneuploidy, a condition where an embryo possesses an abnormal number of chromosomes. The issue remains that the body recognizes these chromosomal anomalies, which explains why the risk of early miscarriage rises from roughly 12 percent for a 20-year-old to approximately 25 percent at age 35. It is a biological tax on time, yet it is far from an absolute barrier to a healthy delivery.
The Role of Cellular Energy and Mitotic Spindles
To understand why egg quality degrades, we must peer into the mitochondria, the tiny cellular powerhouses responsible for generating adenosine triphosphate. Older eggs simply possess less cellular energy to fuel the complex machinery that pulls chromosomes apart during fertilization. When the mitotic spindle fibers slacken due to energy depletion, chromosomes get misallocated. As a result: conditions like Down syndrome, which occurs in about 1 in 1,250 births at age 25, see an increased statistical probability to 1 in 350 at age 35.
How Follicle-Stimulating Hormone Tells the True Story
Chronological age is a blunt instrument, whereas biological markers offer precision. Endocrinologists rely on a battery of tests including Anti-Müllerian Hormone levels and antral follicle counts to gauge the true state of your reproductive engine. A 37-year-old woman with robust AMH levels might possess a significantly easier path to conception than a 31-year-old dealing with premature ovarian insufficiency. People don't think about this enough when obsessing over their birthdays.
Maternal Health Dynamics: Gestational Risks Beyond the Ovaries
Conception represents only the first hurdle because a changing body also alters how it manages a nine-month gestation. Carrying a child strains the cardiovascular system, forcing the heart to pump 50 percent more blood volume by the second trimester. After 35, the vascular system possesses less elasticity, which directly increases the incidence of gestational hypertension and preeclampsia. Preeclampsia—a dangerous spike in blood pressure accompanied by protein in the urine—requires careful vigilance; its incidence climbs by nearly 50 percent in older cohorts compared to women in their twenties.
The Metabolic Shift: Gestational Diabetes Mellitus
Insulin resistance naturally intensifies as we age. When you superimpose the metabolic demands of a growing placenta—which actively secretes hormones that block insulin action—the pancreas occasionally fails to keep pace. Statistics show that the risk of developing gestational diabetes more than doubles once a pregnant individual crosses the 35-year mark. But managed with a rigorous nutritional framework and monitoring, this complication rarely derails a successful birth outcome.
Natural Conception vs. Assisted Reproductive Technology: The True Success Rates
When the traditional route stalls, many assume Reproductive Endocrinology and Infertility clinics offer a guaranteed safety net. I must emphasize that while technology achieves miracles, it cannot entirely reverse the cellular aging of gametes. Data from the Society for Assisted Reproductive Technology reveals that for women under 35, the live-birth rate per single embryo transfer sits comfortably around 45 to 50 percent. By age 37, that metric slips closer to 35 percent. Except that numbers never tell the whole story. A landmark 2019 trial in Copenhagen demonstrated that utilizing preimplantation genetic testing allows embryologists to select only euploid, or chromosomally normal, embryos. When transferring a genetically screened embryo, a 38-year-old achieves nearly the same implantation success rate as a 28-year-old. In short: science has decoupled uterine age from egg age, reshaping the entire landscape of modern parenthood.