We talk about these things as if they are ticking time bombs, but that metaphor is actually quite lazy because bombs have timers and aneurysms have physics. Think of a garden hose with a persistent, bulging blister that just refuses to hold its shape under the summer sun. Eventually, the structural integrity of the rubber reaches a mathematical tipping point. When people ask about the bleeding site, they are often looking for a roadmap to a catastrophe that has already happened. The thing is, by the time the blood is actually leaving the vessel, the "where" becomes a frantic question for a neurosurgeon or a vascular specialist trying to clamp off a high-pressure geyser. Most folks assume you just bleed "inside," yet the specific anatomical compartments that catch this blood determine whether you walk away or become a statistic in a medical journal.
The Structural Anatomy of a Blowout: What an Aneurysm Actually Is
An aneurysm is not a disease in the traditional sense, but rather a localized permanent dilation of an artery that exceeds its normal diameter by at least 50 percent. It is a failure of the tunica media, which is the muscular middle layer of your arterial walls that handles the rhythmic thumping of your heart. When this layer degrades—thanks to a cocktail of genetics, high blood pressure, or perhaps a lifetime of smoking—the artery stretches thin. You might have a saccular aneurysm, which looks like a lone cherry hanging off a branch, or a fusiform aneurysm, where the entire pipe bulges out like a snake that just swallowed a large rodent. But where does the blood go? Because the location of the weakness dictates the path of the flood, we have to look at the surrounding geography.
The Intracranial Compartment and the Circle of Willis
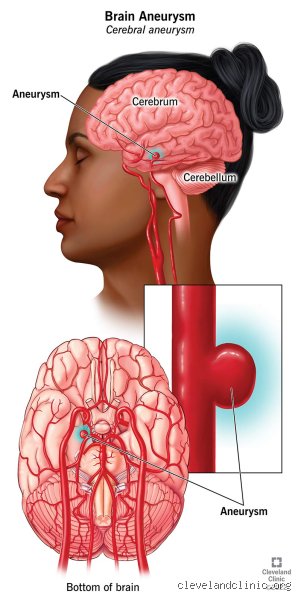
Most brain aneurysms occur in the Circle of Willis, a ring-like junction of arteries at the base of the brain that looks like something designed by a nervous engineer trying to ensure backup power lines. When a leak happens here, the blood doesn't just soak into the brain tissue immediately. Instead, it sprays into the subarachnoid space, which is the fluid-filled gap between the arachnoid membrane and the pia mater. This results in a Subarachnoid Hemorrhage (SAH). It is a sudden spike in intracranial pressure that can shut down vital functions in seconds. Honestly, it’s unclear why some people develop these at the bifurcations—the forks in the road—while others with identical blood pressure remain perfectly intact. Experts disagree on the exact mechanical triggers, but the sheer velocity of the blood entering that tight space is what causes the infamous "thunderclap headache."
Mapping the Hemorrhage: The Three Primary Bleed Zones
Where you bleed is dictated by the specific "neighborhood" of the artery. If we are talking about the chest or abdomen, the Aorta is the primary suspect. As the largest vessel in the human body, the aorta carries a staggering amount of volume. An Abdominal Aortic Aneurysm (AAA) usually occurs below the kidneys. If this ruptures, the blood pours into the retroperitoneal space. This is a hidden area behind the abdominal cavity. Imagine a basement flooding behind a locked door; you might not see the water, but the pressure is destroying the foundations. The sheer volume of blood lost in a Type A dissection or a ruptured AAA can exceed 2 to 3 liters in a matter of minutes, leading to rapid hypovolemic shock. That changes everything for the first responders who have to move faster than the speed of a falling blood pressure cuff.
The Retroperitoneal Versus Intraperitoneal Divide
Where it gets tricky is when the rupture isn't contained by the back wall of the abdomen. If the aneurysm breaks through the peritoneum, the blood enters the actual abdominal cavity where your organs live. This is usually fatal within minutes because there is no pressure from surrounding tissues to help tamponade, or slow down, the flow. Statistics from the Society for Vascular Surgery suggest that while nearly 200,000 Americans are diagnosed with an AAA annually, the rupture mortality rate remains stubbornly high, often exceeding 80 percent for those who don't reach a surgical suite. And even if they do reach the hospital, the surgeons are fighting against a clock that doesn't care about their expertise. Because the aorta is under such high pressure, the bleeding is less of a "leak" and more of a catastrophic structural collapse. Why do we focus so much on the abdomen? Simply because it is the most common site for these large-scale failures outside of the cranium.
The Pericardial Tamponade Risk in Thoracic Failures
In the chest, the geography is even more cramped. A Thoracic Aortic Aneurysm (TAA) might bleed into the mediastinum, which is the space between your lungs. But the real nightmare scenario is when the bleed occurs near the heart and fills the pericardial sac. This is the leathery bag the heart sits in. If blood fills this bag, the heart can't expand to take in more blood. It’s called cardiac tamponade. The heart is literally strangled by the blood that was supposed to be inside the vessels. We are far from a simple solution here, as the surgical intervention required to fix a TAA involves stopping the heart and bypass machines, a feat of medical bravado that was unthinkable before the 1950s.
Cerebral Rupture Mechanics: The Subarachnoid Flood
Back in the skull, the "where" is even more constrained by bone. Since the skull is a rigid box, there is nowhere for the extra blood to go. When you bleed from an aneurysm in the brain, the blood often mixes with Cerebrospinal Fluid (CSF). This mixture is toxic to the brain cells it touches. I’ve seen cases where the initial bleed is small—a "sentinel leak"—that causes a mild headache before the big one hits. Yet, people often ignore these warnings because, let's be honest, who hasn't had a bad headache? But that small spray of blood is a warning shot. In about 85 percent of non-traumatic subarachnoid hemorrhages, a ruptured berry aneurysm is the culprit. These tiny, pea-sized defects usually sit at the base of the brain, waiting for a spike in pressure to let go. As a result: the brain is essentially bruised from the inside out by the sheer force of the arterial jet.
The Difference Between Intracerebral and Subarachnoid Bleeding
People don't think about this enough, but not all brain bleeds are the same. An intracerebral hemorrhage is when the blood actually enters the brain tissue itself, like a bruise inside a peach. An aneurysm, however, is typically on the surface of the vessels, so it bleeds into the spaces around the brain first. Does it matter? Absolutely. The treatment for a bleed in the parenchyma (the functional tissue) is vastly different from coiling or clipping an aneurysm in the subarachnoid space. But the issue remains that any blood outside the vessel in the skull is an emergency. The blood itself causes vasospasm, where other nearby arteries freak out and tighten up, starving the brain of oxygen. It’s a secondary disaster that happens days after the initial bleed, showing that where you bleed is only the first chapter of the crisis.
Comparing Aortic and Cerebral Bleeding Patterns
If we compare a brain bleed to an aortic bleed, the differences are purely about volume versus pressure. A brain aneurysm might only release 30 to 50 milliliters of blood, but because it is inside the skull, that tiny amount is enough to cause a coma or death. In contrast, an aortic aneurysm requires liters of blood loss to achieve the same lethality, simply because the body's trunk can expand and accommodate the fluid—at least for a little while. Historically, surgeons like Michael DeBakey in the mid-20th century revolutionized how we view these sites, moving from "wait and see" to aggressive grafting. Except that even with modern imaging, many of these bleeds are found only during an autopsy because they were asymptomatic until the moment of rupture. The comparison is grim: one is a pressure-cooker explosion in a small box, and the other is a massive pipe burst in a large warehouse. Both are equally effective at ending a life if the "where" isn't addressed within the golden hour of trauma care.
Common mistakes and medical fallacies
People often imagine a cerebral hemorrhage as a slow, trickling leak that produces a dull, nagging ache over several days. The problem is that reality is far more violent. A ruptured intracranial aneurysm does not loiter; it detonates. Many patients mistakenly assume that if they can still walk or talk, they are not currently experiencing a life-threatening bleed. Let's be clear: a subarachnoid hemorrhage can manifest as the most excruciating headache of your life, often described as a thunderclap headache, reaching peak intensity within sixty seconds. Because the blood enters the space surrounding the brain rather than the brain tissue itself initially, focal weakness might be absent, leading people to downplay the catastrophe. Statistics suggest that roughly 25% of patients with this specific presentation are initially misdiagnosed when they seek primary care for what they assume is a standard migraine.
The myth of the warning leak
You might have heard of a sentinel bleed, which is a minor precursor to a major rupture. Yet, these are not gentle nudges from your circulatory system. Even a small amount of blood escaping the arterial wall into the cerebrospinal fluid triggers a massive inflammatory response. Expecting a manageable warning is a gamble where the stakes are your entire cognitive future. Data indicates that among those who experience a sentinel headache, a full-blown rupture follows in 30% to 50% of cases within the subsequent weeks. But waiting for a second, larger event is a recipe for permanent neurological deficit. If you are wondering where do you bleed from an aneurysm, the answer is usually into the subarachnoid space, which quickly increases intracranial pressure and can lead to a rapid loss of consciousness.
Misinterpreting blood pressure spikes
Another frequent error involves the relationship between hypertension and the vascular wall. While chronic high blood pressure weakens the vessel over decades, the moment of rupture is often sparked by a sudden, acute spike in transmural pressure. This explains why heavy lifting, intense emotional stress, or even a vigorous sneeze can be the final straw for a thinned- arterial dome. It is not just about having high numbers on a random Tuesday. The issue remains that the structural integrity of the aneurysm is a ticking clock, and assuming you are safe because your resting pulse is low is a dangerous oversimplification. In short, the vessel doesn't care about your average; it only cares about the peak.
The hemodynamic reality of the Circle of Willis
To understand the mechanics of the rupture, we must look at the Circle of Willis, a pentagonal circuit of arteries at the base of the brain. This is where 85% of all intracranial aneurysms reside. Why? Because fluid dynamics are brutal. As blood rushes through the internal carotid arteries, it hits bifurcations—forks in the road—with immense force. As a result: the constant shear stress wears down the internal elastic lamina. This isn't a flaw in your design so much as a consequence of high-pressure mammalian life. Which explains why the most common site for a bleed is the Anterior Communicating Artery, representing about 30% of cases. (It is quite ironic that the very system designed to ensure redundant blood flow to the brain is the same one that creates the most lethal structural weak points).
The role of the subarachnoid space
When the wall finally fails, the blood doesn't just sit there. It mixes with the cerebrospinal fluid (CSF), which circulates throughout the entire spinal column and brain exterior. This explains the classic symptom of nuchal rigidity or a stiff neck. You aren't just bleeding in your head; you are polluting the entire hydraulic system that cushions your central nervous system. This chemical meningitis caused by free-floating hemoglobin is what causes the long-term vasospasm that can lead to secondary strokes days after the initial bleed has stopped. Expert intervention focuses heavily on managing this toxic environment after the initial "plumbing" fix is completed.
Frequently Asked Questions
Can an aneurysm bleed into the brain tissue itself?
Yes, although the primary location is the subarachnoid space, a high-pressure rupture can tear through the brain's parenchyma. This is known as an intracerebral hemorrhage and occurs in approximately 20% to 40% of ruptured cases depending on the aneurysm's orientation. When this happens, the blood forms a localized clot or hematoma that physically displaces brain cells. This specific type of bleed is often more likely to cause immediate paralysis or speech loss because it strikes the "wiring" directly. Medical imaging like a CT scan will show a dense white mass within the gray matter, signifying a much more complex surgical challenge.
What is the survival rate after a rupture occurs?
The numbers are sobering, as roughly 15% of patients die before they even reach a hospital. For those who do make it to a trauma center, the 30-day mortality rate hovers around 40%. Recovery is a long road, with about one-third of survivors living with permanent neurological impairment that requires ongoing therapy. However, advancements in endovascular coiling and flow diversion have significantly improved outcomes compared to two decades ago. Early detection of an unruptured lesion remains the most effective way to avoid these grim statistics entirely.
Does every aneurysm eventually bleed?
Surprisingly, the answer is no, and many people live their entire lives with a "silent" bulge that never fails. The annual risk of rupture for a small aneurysm—typically under 7 millimeters—is often cited as less than 1% per year. Factors like smoking, a family history of subarachnoid hemorrhage, and the specific shape of the sac (daughter sacs or irregular lobes) increase that percentage. Doctors use the PHASES score to calculate whether the risk of surgery outweighs the risk of the vessel bursting. It is a delicate balance of probability versus the catastrophic reality of a cerebral aneurysm failure.
The imperative of immediate action
We must stop treating the brain's vascular health as a secondary concern that can wait for an annual checkup. When a vessel fails, every second that passes is a literal loss of thousands of neurons that you will never get back. If you feel that sudden, agonizing pop in your skull, do not call your therapist or your mother; you call emergency services immediately. The medical community has become incredibly adept at "plugging the leak" through microvascular clipping or platinum coiling, but we cannot fix dead tissue. I take the firm stance that universal screening for those with two or more first-degree relatives affected should be mandatory. It is time to stop being reactive about where do you bleed from an aneurysm and start being proactive about the structural integrity of our own anatomy. Waiting for the explosion is not a medical strategy; it is a tragedy in progress.