The Anatomy of a Rupture: Defining the Aneurysmal Subarachnoid Hemorrhage
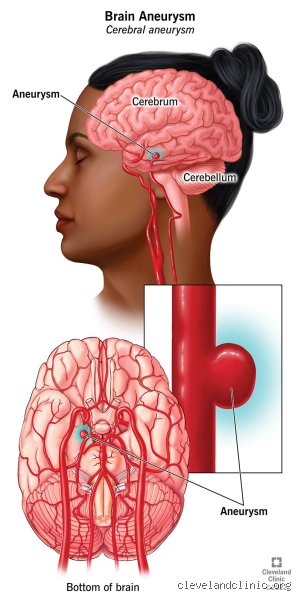
To grasp the prognosis for aneurysmal bleed, you have to understand that we aren't just talking about a headache; we are talking about a structural failure of a cerebral artery. Most of these occur at the Circle of Willis, a crossroads of vessels at the base of the brain where hemodynamic stress is at its peak. Imagine a garden hose with a weak spot that finally gives way under high pressure. That is the aneurysm. When it pops, blood floods the subarachnoid space—the area between the arachnoid membrane and the pia mater—sending intracranial pressure skyrocketing. The thing is, the brain doesn't like being bathed in blood, as the resulting chemical irritation causes the blood vessels to spasm, leading to secondary strokes. That is where it gets tricky for doctors trying to predict an outcome.
The Hunt and Hess Scale and Why It Matters
Clinicians don't just guess at an outcome; they use the Hunt and Hess scale, a five-level grading system created in 1968 that remains the gold standard for predicting mortality. A Grade I patient might just have a slight headache or a stiff neck, and their prognosis for aneurysmal bleed is actually quite favorable, with survival rates often exceeding 70 percent. But move the needle to Grade V—where the patient is in a deep coma or exhibiting decerebrate posturing—and the survival rate plummets toward 10 percent. Is it perfect? No. But it gives us a baseline for the chaos. I’ve seen patients arrive looking relatively stable only to deteriorate within hours because of a re-bleed, which carries a staggering 70 to 90 percent mortality rate if it happens before the aneurysm is secured.
The Statistical Ghost: The Incidence Rate in 2026
People don't think about this enough: the global incidence of aneurysmal subarachnoid hemorrhage (aSAH) sits at about 9 per 100,000 person-years, but these numbers vary wildly by geography. In Finland and Japan, the rates are nearly double, likely due to a cocktail of genetic predisposition and high hypertension rates. If you are a smoker or have uncontrolled high blood pressure, you are effectively living with a ticking clock in your cranium. Yet, despite these terrifying odds, the case fatality rate has actually dropped by about 1 percent per year over the last few decades. We're far from a "cure," but the survival curve is finally bending in the right direction.
Immediate Clinical Trajectory: The First 72 Hours of Survival
The first three days are a gauntlet. Once the patient survives the initial aneurysmal bleed, the primary goal is "securing the dome"—either via endovascular coiling or microsurgical clipping—to prevent that dreaded second rupture. During this window, the prognosis for aneurysmal bleed is largely determined by the volume of blood seen on a CT scan, often measured by the Fisher Grade. A thick layer of blood in the cisterns usually signals a high risk of delayed cerebral ischemia (DCI). But here is the nuance: even if the surgery goes perfectly, the brain remains in an inflammatory state that can last for weeks.
The Triple-H Therapy Controversy
For years, the standard of care was "Triple-H therapy"—hypervolemia, hemodilution, and induced hypertension—to keep blood flowing through vasospastic vessels. Experts disagree on its efficacy now. Recent studies suggest that simply maintaining euvolemia (normal fluid levels) and using Nimodipine, a calcium channel blocker, is just as effective without the risk of pulmonary edema or heart failure. The issue remains that we are trying to force blood into a brain that is actively trying to shut down its own supply lines. It’s a delicate balancing act that requires 24-hour monitoring in a specialized Neuro-ICU, a factor that significantly improves the prognosis for aneurysmal bleed compared to general intensive care units.
The Role of Hydrocephalus in Early Recovery
About 20 to 30 percent of patients develop acute hydrocephalus because the blood prevents the normal drainage of cerebrospinal fluid. This causes the ventricles to enlarge, crushing brain tissue from the inside out. A quick fix involves placing an External Ventricular Drain (EVD), a plastic tube that snakes into the brain to let the fluid out. And while this can save a life in minutes, it also introduces a risk of infection or "ventriculitis." Which explains why some patients seem to be recovering only to hit a wall due to a secondary hospital-acquired complication.
Secondary Complications and the Vasospasm Window
If you make it past day three, you enter the "vasospasm window," which typically peaks between days 7 and 10. This is the period where the prognosis for aneurysmal bleed can take a sharp turn for the worse. The blood products from the initial rupture begin to break down, releasing irritating substances that cause the brain's arteries to narrow. Think of it like a localized drought; the territory downstream of the spasm starts to die. Because of this, patients who seemed perfectly lucid on day four might suddenly lose the ability to speak or move their right side by day eight. That changes everything for the family and the long-term outlook.
Monitoring the invisible with Transcranial Doppler
To catch these spasms before they turn into permanent strokes, we use Transcranial Doppler (TCD) to measure the velocity of blood flow through the Middle Cerebral Artery. High velocities suggest the vessel is narrowing. In short, the faster the blood has to move to get through the gap, the more worried the neurosurgeon becomes. Some centers are now using continuous EEG monitoring to look for "spreading depolarizations"—electrical storms in the brain that correlate with poor prognosis for aneurysmal bleed and might actually be more predictive than traditional imaging. It’s a high-tech game of cat and mouse.
Ischemic Brain Injury: The Silent Prognosis Killer
Even if no overt vasospasm is detected, we now know about microthrombi—tiny blood clots that form in the smallest vessels of the brain after a hemorrhage. These don't show up on a standard CT scan, yet they cause diffuse damage that leads to cognitive "fog," memory loss, and executive dysfunction. Honestly, it's unclear why some brains tolerate this better than others. But we do know that patients with higher levels of biomarkers like S100B or neuron-specific enolase in their blood usually face a steeper climb in rehabilitation. Data from a 2025 multi-center trial in Lyon showed that early intervention with anti-platelet therapy might mitigate this, though the bleeding risk makes most surgeons nervous.
Clipping vs. Coiling: Does Method Impact Long-term Prognosis?
One of the biggest debates in neurosurgery is how the method of repair affects the prognosis for aneurysmal bleed. The International Subarachnoid Aneurysm Trial (ISAT) famously suggested that endovascular coiling—where a catheter is threaded from the groin to the brain—resulted in better one-year outcomes than microsurgical clipping, which requires a craniotomy. However, coiling has a higher rate of aneurysm recurrence. If the coils settle and the aneurysm regrows, the patient faces a lifelong risk of a second bleed. As a result: younger patients often opt for the "one and done" nature of the clip, even if the initial recovery is more brutal.
The Cognitive Trade-off of the Craniotomy
Opening the skull is inherently traumatic. While clipping is more definitive for the prognosis for aneurysmal bleed, the retraction of brain tissue can lead to localized bruising. Compare this to coiling, where the brain isn't touched directly, but the patient must remain on blood thinners for a period, which has its own set of dangers. It is a choice between the immediate safety of the procedure and the long-term security of the repair. Except that for some complex, wide-necked aneurysms, coiling isn't even an option, making the debate moot for a large portion of the population.
Common Mistakes and Misconceptions Regarding Post-Hemorrhage Outcomes
The Fallacy of the "Safe" Silver Coil
Many families assume that once a surgeon navigates the femoral artery to deploy platinum coils or a flow-diverter stent, the danger has evaporated. It has not. While endovascular coiling successfully prevents a second catastrophic rupture, it does nothing to clear the subarachnoid space of caustic, degrading blood. Let's be clear: the procedure secures the structural defect, but the biochemical assault on the brain tissue is only beginning. You might see a perfect radiological result on a post-op angiogram while the patient remains in a deep coma. Because the blood breakdown products, specifically oxyhemoglobin, trigger a massive inflammatory cascade, the technical success of the "fix" does not dictate the immediate prognosis for aneurysmal bleed. It is a common error to conflate mechanical repair with neurological recovery.
Misinterpreting the Stability of "Grade I" Patients
The Hunt and Hess scale often lulls clinicians and relatives into a false sense of security when a patient arrives awake and oriented. But the issue remains that even those with a Grade I or II presentation face a 20 percent to 30 percent risk of developing delayed cerebral ischemia (DCI) between day four and day fourteen. We often witness a "talk and die" scenario where an initially stable patient suffers a massive stroke a week later due to vasospasm. The problem is that clinical stability is a snapshot, not a movie. Why do we treat these patients as out of the woods before the ten-day mark? If you ignore the delayed physiological window, you are essentially gambling with a 30 percent risk of secondary infarction despite an initially "good" status. As a result: vigilance must be absolute regardless of the initial clinical score.
The Hidden Architect of Survival: The Glymphatic Clearance Factor
Beyond the Vessel: The Role of Waste Clearance
Standard expert advice focuses almost exclusively on arterial diameter and vasospasm. Yet, a little-known aspect of the prognosis for aneurysmal bleed involves the glymphatic system—the brain's internal plumbing. When an aneurysm bursts, it does not just leak; it floods the basement membrane and perivascular spaces with fibrin and cellular debris. This physical "sludge" prevents the normal clearance of metabolic waste. Recent pilot data suggests that patients with impaired glymphatic flow prior to the event (often seen in chronic hypertensives) suffer significantly worse cognitive outcomes. (We rarely measure this, which is a massive oversight in current neuro-critical care). If the brain cannot "flush" the toxic iron deposits left behind by the subarachnoid hemorrhage, neurodegeneration continues long after the ICU discharge. Strengthening sleep hygiene and managing intracranial pressure specifically to favor glymphatic outflow might be the next frontier in improving the long-term recovery outlook. In short, the vessel is the spark, but the plumbing is the fuel.
Frequently Asked Questions
Does the size of the initial aneurysm dictate the chance of a full recovery?
Surprisingly, the correlation between the original dome size and the final prognosis for aneurysmal bleed is less linear than one might expect. While a giant aneurysm (greater than 25mm) carries higher surgical risk, a small 3mm rupture can cause just as much devastating parenchymal damage if the pressure of the jet is high. Data from the ISAT and ISUIA trials indicate that site-specific factors, such as a posterior circulation location, are often more predictive of mortality than sheer diameter alone. Mortality rates for posterior communicating artery ruptures remain stubbornly high, regardless of whether the lesion was small or large. The volume of blood distributed in the cisterns, measured by the Fisher Scale, is a much more reliable metric for predicting neurological deficits than the size of the vessel defect itself.
How long does the risk of "re-bleeding" persist after the first event?
The highest risk for a second rupture occurs within the first 24 hours, with statistics showing that 15 percent to 20 percent of untreated patients will re-bleed in this window. This secondary event is almost always fatal, carrying a mortality rate exceeding 70 percent. Once the aneurysm is successfully clipped or coiled, this specific risk drops to nearly zero, although the patient is never truly "cured" of the underlying vasculopathy. You must understand that after the first year, there is a 1 percent to 2 percent annual risk of a de novo aneurysm forming elsewhere in the Circle of Willis. Which explains why lifelong surveillance via MRA or CTA is mandatory for anyone who has survived a primary aneurysmal subarachnoid hemorrhage.
Can a patient return to a high-stress career after a subarachnoid hemorrhage?
Return to work is possible, yet the statistics are sobering: only about 30 percent to 50 percent of survivors return to their previous level of professional employment within one year. Even in "good outcome" cases, patients frequently struggle with executive dysfunction, emotional lability, and a pervasive "brain fog" that standardized tests often miss. These subtle cognitive impairments are frequently the result of diffuse axonal injury caused by the initial pressure spike at the moment of rupture. It is not just about moving your arms and legs; it is about the high-level processing required for complex decision-making. Vocational rehabilitation must start early, focusing on compensatory strategies for memory and attention rather than just physical strength.
The Verdict: Rethinking Post-Bleed Success
We need to stop defining "success" merely as the absence of a corpse. The medical community often celebrates a favorable prognosis for aneurysmal bleed when a patient walks out of the hospital, ignoring the fact that their personality might be shattered or their cognitive stamina non-existent. My position is firm: we are over-invested in the acute surgical "fix" and dangerously under-invested in the chronic neuro-inflammatory phase. Expecting a human to return to "normal" after their brain has been bathed in caustic blood is a medical fantasy. Except that we continue to use blunt metrics like the Modified Rankin Scale to justify discharging patients into a vacuum of care. True prognosis is a multi-year trajectory, not a two-week ICU stay. We must prioritize the long-term biochemical cleanup of the brain if we ever hope to move the needle on quality of life. Until we treat the bleed as a systemic neurological disease rather than a localized plumbing failure, our "miracles" will remain tragically incomplete.