Beyond the Stethoscope: Why We Still Rely on Physical Assessment in the Digital Age
The thing is, we have become dangerously reliant on the "donut of truth"—the CT scanner—to tell us what is wrong with the human body, yet a seasoned practitioner can often reach a diagnosis using nothing but their own five senses. It sounds almost archaic, right? But the reality is that the physical examination provides immediate, real-time data that no blood test can replicate, especially during that first high-stakes interaction in an emergency department or a rural clinic where power is a luxury. We are witnessing a slow erosion of these skills, which I find frankly alarming, as the digital screen creates a physical barrier between the doctor and the person sitting in front of them.
The Historical Weight of the IPPA Sequence
The issue remains that students often view these methods as a hurdle to pass for their board exams rather than a diagnostic lifeline. It wasn't until the late 18th and early 19th centuries that figures like Leopold Auenbrugger (the father of percussion) and René Laennec (the inventor of the stethoscope) codified these movements into a rhythmic dance of diagnostic discovery. Because medicine is as much a craft as it is a science, the sequence matters. If you press on a patient’s belly before looking at it, you might induce muscle guarding or change the bowel sounds you’re about to hear, effectively muddying the diagnostic waters before you've even started. Yet, even with this history, experts disagree on whether we should prioritize newer ultrasound technologies over the traditional tactile approach.
A Shift in Clinical Philosophy
Where it gets tricky is balancing the speed of modern healthcare with the deliberate pace required for a thorough physical. Some argue that the "physical exam is dead," replaced by point-of-care ultrasound (POCUS), but we’re far from it being a universal replacement. Palpation and inspection offer a level of intimacy and trust-building that a cold probe on the skin simply cannot match. Which explains why, despite the influx of AI-driven diagnostics, the hands-on approach remains the most cost-effective way to filter out the noise from the signal in a complex clinical presentation.
Inspection: The Silent Power of the First Glance
Most people don't think about this enough, but the examination begins the very second you walk into the room. Inspection is the first of the 4 ways to examine a patient, and it is far more than just "looking"—it is a disciplined, systematic observation that requires the clinician to be hyper-aware of symmetry, color, and movement. Is the patient leaning forward to breathe (the tripod position)? Is there a subtle icteric yellowing of the sclera that hints at liver failure? If you miss the slight jugular venous distention because you were too busy looking at the chart, you’ve already failed the most passive part of the exam.
Systematic Observation Versus Casual Looking
True inspection requires adequate lighting and, quite honestly, the courage to ask a patient to disrobe appropriately. (Nothing hides a brewing cellulitis or a suspicious melanoma better than a thick wool sweater). You are looking for things that don't belong, such as ecchymosis, scars from forgotten surgeries, or the rhythmic "water-hammer" pulse in the neck that screams aortic regurgitation. This isn't just about the skin; it’s about the way the chest expands—or doesn't—during a deep breath. But here is where it gets interesting: the most skilled observers can spot a Parkinsonian tremor or the "mask-like" facies of a neurological disorder before the patient has even finished their first sentence.
The Role of Symmetry in Clinical Deduction
And then there is the rule of halves. The human body is remarkably symmetrical, which makes unilateral edema in a single leg a massive red flag for a Deep Vein Thrombosis (DVT). Why would one calf be 3 centimeters larger in circumference than the other? As a result: the clinician must constantly compare the left side to the right, using the patient’s own anatomy as the "control group" for the experiment. It is a visual puzzle where the pieces are often hidden in plain sight, waiting for someone with a trained eye to notice the slight deviation from the norm.
Palpation: When the Hands Become Diagnostic Instruments
Once the eyes have done their work, the hands take over. Palpation is the second stage of the 4 ways to examine a patient, involving the use of touch to determine the texture, temperature, and crepitus of underlying structures. There is a specific geography to the hand: the finger pads are for fine tactile discrimination (like feeling a pulse), while the ulnar surface or palms are better for sensing vibrations or "thrills" over the heart. But wait, did you remember to warm your hands first? Cold hands are the fastest way to trigger voluntary guarding, which is a muscular contraction that makes it impossible to feel the organs beneath the surface.
Deep Versus Superficial Pressure
We generally divide this into two distinct depths. Light palpation, usually pressing down about 1 centimeter, is used to check for tenderness or surface masses. Deep palpation, which can reach 4 to 5 centimeters, is necessary to locate the lower border of the liver or the poles of the kidneys. Honestly, it’s unclear to many novices how much pressure is "too much," but the patient's face usually provides the answer before their voice does. That changes everything, because if you see a wince, you’ve found a focal point of pathology, perhaps McBurney’s point tenderness, which has been a hallmark of appendicitis since 1889.
Assessing Temperature and Moisture
The back of the hand—the dorsal surface—is the body's most sensitive thermometer. It can detect the subtle heat of a localized infection or the "clammy" skin of someone sliding into hypovolemic shock. Yet, palpation is not just about finding what is there; it is about confirming what is missing. The absence of a dorsalis pedis pulse in the foot can be the first indicator of peripheral artery disease, potentially saving a limb from future amputation. In short, your hands are capable of measuring turgor, identifying lymphadenopathy, and feeling the "heave" of an enlarged heart, all without a single watt of electricity.
The Evolution of Assessment: Traditional IPPA vs. The Modern Ultrasound
There is a brewing civil war in medical education regarding the 4 ways to examine a patient. On one side, you have the purists who believe that the acoustic stethoscope is an extension of the doctor’s soul. On the other, you have the "POCUS" advocates who argue that looking at the heart with sound waves is objectively superior to listening to it. It’s a compelling argument—a 2018 study suggested that medical students using portable ultrasound could identify cardiac pathology more accurately than experienced cardiologists using only a stethoscope. But the issue remains: what happens when the battery dies? Or when you’re in a disaster zone with no equipment?
Technology as a Complement, Not a Replacement
I would argue that the best clinicians use technology to confirm their physical findings, not to bypass the exam entirely. If you feel a pulsatile mass in the abdomen during palpation, you are already 90% of the way to diagnosing an Abdominal Aortic Aneurysm (AAA). The ultrasound just gives you the measurements. Except that many young residents now skip the palpation and go straight to the scan, which leads to a loss of the "clinical intuition" that comes from touching thousands of patients. This trend is a double-edged sword; we gain precision but lose the holistic view of the person as a biological whole rather than a collection of pixelated slices.
The Pitfalls of Surface-Level Assessment
Modern clinicians often stumble because they treat the physical exam as a checklist rather than a narrative. The problem is that technology has bred a sort of diagnostic laziness where the hands-on 4 ways to examine a patient are viewed as vestigial relics of a pre-MRI era. We see this most clearly in the rushed auscultation. Most practitioners spend less than 2 seconds per valve area, yet a study from the American Journal of Medicine suggests that detecting a Grade II systolic murmur requires at least 15 seconds of focused auditory concentration to filter out background noise. You cannot find what you are not looking for. If you approach the body like a grocery list, you will miss the subtle clues.
The False Security of Equipment
But there is a deeper issue regarding the over-reliance on digital tools. Let's be clear: a pulse oximeter is not a replacement for palpation. Relying solely on the screen leads to a phenomenon known as "clinical myopia" where the practitioner ignores the capillary refill time because a sensor gave a numerical value. A cold, clammy hand tells a story of peripheral vasoconstriction that a 98% saturation reading might mask in early stages of shock. The issue remains that we are losing the tactile intuition required to sense the rigidity of a peritoneal abdomen, which no ultrasound can truly replicate in terms of immediate feedback. Except that we keep pretending the machine is smarter than the fingers.
Misinterpreting Symmetry
Which explains why many beginners fail to compare bilateral structures correctly. It is not enough to palpate the right radial pulse; you must synchronize it with the left to detect a subclavian steal or coarctation. We often see students performing percussion on the chest without a "ladder" pattern. As a result: they miss the shifting dullness of a small pleural effusion because they have no baseline for that specific patient's resonance. You must be the calibrator.
The Hidden Rhythm of Non-Verbal Data
There is a clandestine layer to the clinical assessment process that textbooks rarely quantify. It is the "smell of the disease." Experienced veterans know that pseudomonas infections carry a distinct, sickly sweet grape odor, while diabetic ketoacidosis presents with a fruity, ketotic breath that a standard physical examination might not officially list in the four-point protocol. This is the art. It is the ability to integrate olfactory data with the tactile fremitus felt during palpation.
The Power of the Silent Minute
The best expert advice is surprisingly simple: stop talking. (Wait, is it actually possible for a doctor to be quiet for sixty seconds?) When you begin the inspection phase, the patient’s gait, the way they hold their neck, and the symmetry of their facial folds provide 70% of the diagnosis before you even reach for the stethoscope. In short, the physical exam begins the moment you enter the room, not when the patient unbuttons their shirt. Research indicates that 80% of medical errors are related to cognitive biases formed in the first 30 seconds of an encounter. By forcing yourself into a minute of pure observation, you bypass the urge to jump to conclusions based on the chief complaint alone. Yet, how many of us actually have the discipline to just watch?
Frequently Asked Questions
Can digital tools replace the traditional physical examination?
The short answer is a resounding no, despite the influx of handheld ultrasound devices and AI-driven diagnostic aids. While a 2023 study published in The Lancet showed that point-of-care ultrasound (POCUS) increased diagnostic accuracy by 22% in emergency settings, it functioned as an adjunct rather than a replacement. The human touch provides psychological reassurance that a cold metal probe cannot offer. Furthermore, the 4 ways to examine a patient allow for the detection of subtle nuances, like the texture of a skin lesion or the specific "catch" in a joint's range of motion, which sensors often overlook. We must view technology as an extension of our senses, not a substitute for them.
How long should a comprehensive physical exam take in a primary care setting?
Time is a luxury, but quality requires a specific minimum. A standard, focused physical exam typically lasts between 8 to 12 minutes, though a comprehensive head-to-toe assessment can easily extend to 20 minutes if performed with the requisite depth. Data from the Journal of General Internal Medicine indicates that the average primary care visit lasts only 15.7 minutes in total. This creates a dangerous "time-crunch" where percussion and palpation are often truncated to save time. Because of these constraints, clinicians must become more efficient, moving through the inspection and auscultation phases with a practiced, fluid motion that maximizes every second of patient contact. Efficiency is not the same as rushing.
What is the most commonly missed finding during the four-step process?
Statistically, the most frequently overlooked signs occur during the inspection of the posterior thorax and the lower extremities. Many practitioners fail to ask the patient to stand or turn around, meaning they miss sacral edema or early-stage pressure ulcers. In dermatological screenings, nearly 35% of malignant melanomas are found in areas the patient cannot easily see, necessitating a thoroughness that many "abbreviated" exams lack. The problem is that we focus on the front of the body because it is easier to access. But a complete physical diagnostic evaluation requires a 360-degree view of the human form to be truly effective. If you don't look, you won't find.
The Verdict on Hands-On Medicine
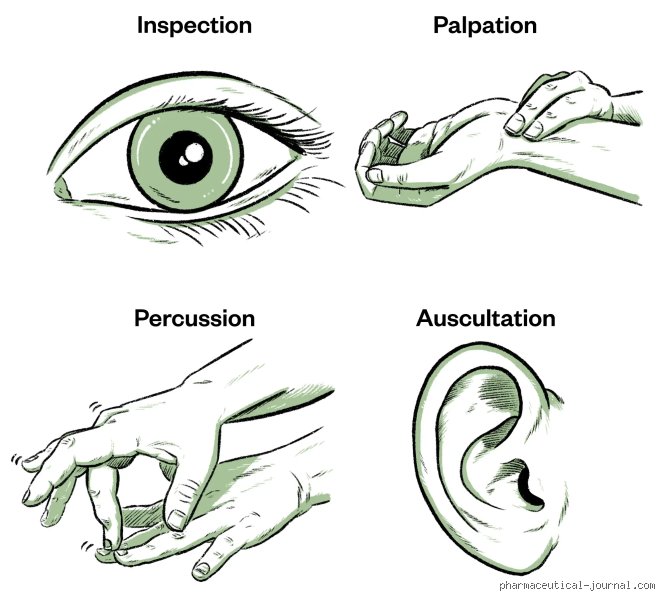
The death of the physical exam has been greatly exaggerated by those who prefer data points to people. I take the firm position that the stethoscope is not a costume piece for a LinkedIn profile; it is a vital tool of sensory integration. We have become far too comfortable letting lab results dictate the "truth" while ignoring the palpable mass staring us in the face. It is an irony of modern medicine that we have more data than ever, yet we understand the physical reality of our patients less. The four classic techniques of inspection, palpation, percussion, and auscultation are not just methods; they are a philosophy of presence. If you cannot master these, you are not a clinician; you are merely a high-paid data entry clerk with a fancy title. We must return to the bedside or lose the soul of the craft entirely.