The Structural Mirage: Why People Don't Think About This Enough
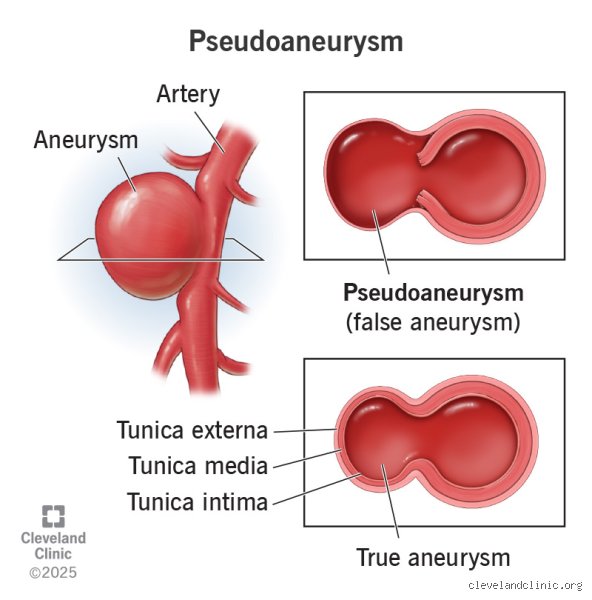
When we talk about vascular health, the term aneurysm usually conjures images of a ballooning vessel wall, a structural weakening that involves all three layers of the artery: the intima, media, and adventitia. But a pseudoaneurysm—or false aneurysm—is a different beast entirely. It occurs when a hole develops in the arterial wall, allowing blood to escape into the surrounding space where it is eventually trapped by a thin, tenuous shell of fibrin and hematoma. Yet, to the untrained eye or even a basic ultrasound, it might look identical to a standard bulge. Except that it isn't. It is essentially a pulsatile hematoma that maintains a direct communication with the high-pressure arterial lumen through a narrow neck.
The Dangerous Anatomy of a False Wall
Most patients encounter this condition following some form of trauma, often iatrogenic, meaning it was caused by a medical procedure like a femoral artery catheterization during a stent placement or an angiogram. But why does the body allow this to happen? Because the pressure inside the artery is so immense that if the puncture site fails to seal, the blood has nowhere to go but out, carving a cavity into the soft tissue. This cavity doesn't have the elastic strength of a real blood vessel. I find it fascinating—and terrifying—that a person can walk around with a pocket of blood held back by nothing more than a bruised layer of fibers. The issue remains that this "wall" is prone to rupture because it lacks the tunica media, the muscular layer that gives our arteries their resilience. Honestly, it's unclear why some people can tolerate these for weeks while others face a rupture within hours, though vessel diameter and systemic blood pressure clearly play the villain here.
Tricky Scenarios: The Femoral Artery and Beyond
Where it gets tricky is in the groin. The femoral artery is the most common site for these lesions, specifically after cardiac interventions involving large-bore sheaths. If you have ever had a "heart cath," your doctor likely checked your groin for a palpable thrill or a rhythmic, vibrating sensation. That vibration is the blood rushing in and out of the pseudoaneurysm neck, a phenomenon often described by radiologists as the "yin-yang sign" on a color Doppler ultrasound. In 2023, data from several vascular registries suggested that the incidence of post-catheterization pseudoaneurysms fluctuates between 0.2 percent and 8 percent depending on the complexity of the procedure and the use of anticoagulants. These numbers might seem low, but for the individual patient, that changes everything.
The Silent Threat of Mycotic Pseudoaneurysms
Not all pseudoaneurysms are born from needles or knives. Some are the result of infection, specifically mycotic pseudoaneurysms, which are far more sinister and harder to manage than their traumatic cousins. These occur when bacteria, often Staphylococcus aureus or Salmonella, settle into a weakened arterial wall and eat away at the tissue. We're far from a simple fix here. Because the tissue is infected, traditional stenting often fails, as placing a piece of metal into an infected field is like throwing gasoline on a fire. This forces surgeons to get creative, sometimes performing extra-anatomic bypasses to reroute blood flow away from the "hot" zone. It is a high-stakes game of vascular chess where the pieces are made of fragile, inflamed tissue.
Visceral and Carotid Anomalies
While the groin is the usual suspect, pseudoaneurysms can hide in the splenic artery or the carotid. A splenic artery pseudoaneurysm is frequently a byproduct of chronic pancreatitis, where digestive enzymes literally digest the neighboring blood vessels. As a result: the patient might feel a vague ache in the upper left quadrant of their abdomen, or they might feel nothing at all until the moment of rupture. In the carotid artery, these lesions often follow a blunt neck injury or a high-velocity car accident. Can you live with a hole in your carotid artery that is only being held shut by a clot? Technically, for a while. But the risk of an embolic stroke is so high that most surgeons won't let the sun go down before proposing a plan of action.
The Survival Spectrum: Stability vs. Catastrophe
The medical community often debates the "wait and watch" approach. For pseudoaneurysms smaller than 2.0 centimeters in the femoral region, many clinicians argue for a conservative path. They believe that if the neck of the lesion is narrow and the patient is not on heavy blood thinners, the blood inside will eventually clot on its own. And they are often right. Statistics show that up to 90 percent of these small, asymptomatic lesions will spontaneously thrombose within four weeks. But this is where I take a sharp opinion: "watching" a pseudoaneurysm in a patient who is non-compliant with bed rest or who has uncontrolled hypertension is medical negligence. You cannot treat a pressurized leak with a "maybe it will go away" attitude if the systemic pressure is pushing 180/100 mmHg. Which explains why blood pressure management is the unsung hero of vascular recovery.
The Role of Compression and Thrombin
In the late 1990s and early 2000s, the standard of care shifted away from open surgery toward ultrasound-guided compression. It was a brutal process—a technician would literally lean on the patient's groin with a transducer for 30 to 60 minutes to force the hole shut. It was painful, exhausting, and had a failure rate hovering around 30 percent. Then came ultrasound-guided thrombin injection (UGTI). This procedure involves sticking a fine needle into the pseudoaneurysm sac and injecting a clotting enzyme. It works almost instantly. The blood turns to a solid plug, the "yin-yang" disappears, and the danger is neutralized. Yet, even this isn't perfect. If the thrombin leaks into the main artery, it can cause a massive clot that cuts off circulation to the entire leg, leading to potential amputation. It is a delicate balance of precision and timing that makes vascular medicine so gripping.
Comparing the True and the False: A Structural Analysis
To understand if you can live with this, you must understand the difference between a true aneurysm and this imposter. A true aneurysm is a chronic condition, often taking years to develop as the elastic fibers in the wall degrade. It is like an old garden hose that is slowly thinning out. A pseudoaneurysm is a hemodynamic crisis disguised as a stable lump. It is a burst pipe where the water is currently being held back by a pile of rags. In short, the "life expectancy" of a pseudoaneurysm is naturally shorter because it lacks the structural integrity to withstand the constant pounding of 70 to 100 heartbeats per minute. While a true aortic aneurysm might be monitored for a decade, a pseudoaneurysm is rarely monitored for more than a month before a definitive "fix or fade" decision is made.
The Patient Experience: Pain and Pulsation
What does it actually feel like to live with one? Most patients describe a deep, boring pain that doesn't respond well to standard analgesics. There is also the psychological toll of feeling your pulse in a place where it shouldn't be—a rhythmic thumping in the thigh or the neck that serves as a constant reminder of the fragility of the vessel. Because the blood is turbulent inside the sac, it often creates a bruit, a whooshing sound that a doctor can hear with a stethoscope. Can you ignore that? Some do, but the physical discomfort usually drives them back to the clinic. The issue remains that the skin over a large pseudoaneurysm can become thin, shiny, and eventually necrotic as the pressure from underneath cuts off the skin's own blood supply. This is the final warning sign before a rupture occurs.
Common mistakes and misconceptions about your arterial bulge
The problem is that many people confuse a true aneurysm with its chaotic, lawless cousin, the pseudoaneurysm. While a genuine aneurysm involves a localized dilation of all three layers of the arterial wall, the false version is actually a contained leak, a hematoma masquerading as a vessel extension. You might think that because the skin looks healed after a catheterization, the internal plumbing is fine. That is a dangerous assumption. Let's be clear: the lack of a visible bruise does not mean the pulsatile mass beneath your femoral artery has vanished into thin air. Many patients assume "living with it" means ignoring it, yet ignoring a high-pressure blood pocket is like keeping a grenade with a loose pin in your pocket. Clinical data suggests that roughly 2% to 6% of cardiac catheterization procedures result in these iatrogenic injuries, yet patients frequently skip their follow-up ultrasounds because they feel fine.
The myth of spontaneous resolution
Because some small leaks do clot off on their own, a pervasive myth exists that time is the only healer you need. It is true that pseudoaneurysms smaller than 2 centimeters might undergo spontaneous thrombosis within four weeks. However, relying on luck is a poor medical strategy. If the neck of the injury is wide, or if you are on anticoagulants like warfarin or clopidogrel, the chances of it closing without intervention drop significantly. Why would you gamble with your circulatory integrity? Waiting too long can turn a simple ultrasound-guided compression into a complex surgical nightmare. As a result: the window for non-invasive repair often closes while you are busy "watching and waiting" for a miracle that biology may not provide.
Misinterpreting the pain signals
Pain is a fickle narrator. You might expect a femoral artery pseudoaneurysm to scream with agony, but it often presents as a dull, rhythmic throb or a strange heaviness in the limb. Some patients misinterpret this as simple post-operative soreness or muscle strain from the hospital bed. But the issue remains that this pressure can actually compress adjacent nerves, leading to numbness or weakness that has nothing to do with your muscles. If the skin starts to thin or turn a dusky blue, you are no longer dealing with a minor inconvenience; you are witnessing impending cutaneous necrosis.
The hidden danger of high-velocity jets
There is a specific, technical nuance that even some general practitioners overlook: the to-and-fro waveform observed during a duplex Doppler exam. This is the hemodynamic signature of the beast. Blood rushes into the false sac during systole and scurries back into the artery during diastole. This constant, high-velocity turbulence prevents the blood from clotting, effectively keeping the "wound" fresh every second of the day. Except that this turbulence also erodes the surrounding tissue. If you are living with a pseudoaneurysm, you aren't just carrying a static lump; you are hosting a dynamic, erosive process that can eventually cause the overlying skin to fail. (This is particularly true in the groin, where movement constantly stresses the site). I firmly believe that any practitioner who suggests "living with" a symptomatic or enlarging lesion without a surgical consultation is flirting with negligence. We have reached a point in vascular medicine where ultrasound-guided thrombin injection has a success rate exceeding 90%, making "watchful waiting" for large lesions look archaic and unnecessarily risky.
The role of physical exertion
You cannot simply return to your marathon training if you have a vascular complication lurking in your thigh or arm. Every spike in blood pressure acts like a hammer blow against the fragile wall of the hematoma. If your systolic pressure hits 160 mmHg during a heavy lift, that pressure is transmitted directly into the pseudoaneurysm sac. Which explains why many "stable" leaks suddenly rupture during mundane activities like straining on the toilet or lifting groceries. We often see patients who were "cleared" for activity too soon, only to return to the ER with a massive internal hemorrhage. In short: your activity level must be strictly dictated by the vascular surgeon, not by how much energy you feel you have.
Frequently Asked Questions
Can a pseudoaneurysm go away on its own without surgery?
Small lesions under 2 or 3 centimeters in diameter can occasionally resolve through spontaneous thrombosis, particularly in patients with normal coagulation profiles. Statistics indicate that up to 40% of small iatrogenic pseudoaneurysms may close within a month of the initial injury. But you must remain under strict ultrasound surveillance during this period to ensure the sac is shrinking rather than expanding. If you are taking blood thinners, the likelihood of this self-healing process decreases to almost zero. It is a waiting game where the stakes are your limb and your life.
What are the signs that a pseudoaneurysm is about to rupture?
The most alarming symptoms include a sudden, sharp increase in pain and a visible expansion of the pulsatile mass under the skin. You might also notice the skin becoming shiny, tight, or significantly discolored, indicating that the pressure is compromising local blood flow. If the limb becomes cold, pale, or difficult to move, the pseudoaneurysm may be causing a "steal syndrome" or compressing the main artery. This is a surgical emergency requiring immediate intervention to prevent permanent nerve damage or tissue loss. Never wait for the pain to become unbearable before seeking help.
How is a pseudoaneurysm treated if it does not heal?
Modern medicine favors ultrasound-guided thrombin injection as the primary gold standard for most accessible leaks. This procedure involves a radiologist injecting a clotting enzyme directly into the sac, which usually hardens the blood within seconds. For cases where the anatomy is too complex or the "neck" is too wide, surgical repair or the placement of a covered stent may be necessary. These interventions boast a high safety profile, often allowing patients to return home the same day. As a result: the morbidity of treatment is far lower than the catastrophic risk of a ruptured arterial wall.
The definitive stance on your vascular health
Living with a pseudoaneurysm is not an exercise in endurance; it is a calculated medical risk that requires constant, expert recalibration. I take the firm position that the "wait and see" approach is overused and often serves as a mask for clinical indecision. You should prioritize definitive closure via thrombin injection or surgery whenever the lesion exceeds a safe threshold or causes even minor discomfort. The biological reality is that a contained arterial leak is an unstable entity that respects no one's schedule. Data proves that early intervention saves limbs and reduces long-term healthcare costs by preventing emergency surgeries. Do not let a manageable vascular complication become a life-altering disaster through medical complacency. Your goal is not to coexist with the bulge, but to eliminate it before it eliminates your peace of mind.