Understanding the DNA of the WHO-5 assessment in clinical practice
When we talk about psychiatric screening, we usually expect a long-winded interrogation that feels more like a deposition than a check-up. The WHO-5 assessment flips that script entirely. It emerged from the Max Hamilton bicentenary meeting in 1995, where researchers realized that the existing tools—specifically the 28-item WHO-10—were simply too bulky for a busy GP to use while a patient is sitting there with a cold. The thing is, clinicians need speed. They need a tool that can be finished in 60 seconds without losing the nuance of a person's internal world. Because the WHO-5 focuses on positive affect rather than the absence of pathology, it sidesteps the immediate stigma often attached to mental health evaluations.
The move from measuring illness to measuring wellness
We spent most of the 20th century obsessed with the "deficit model" of medicine, where you only exist once you are broken. But the WHO-5 assessment was built on the premise of "positive well-being," a concept pioneered by researchers like Per Bech. It doesn't look for the dark shadows of suicidal ideation or clinical lethargy right out of the gate. Instead, it measures your "vitality." Are you waking up refreshed? Have you felt calm and relaxed? This distinction changes everything. It allows the scale to be used in non-clinical settings, like a high-performance workplace or a sports team, where the word "depression" might make people clam up and hide their true state.
The math behind the five simple questions
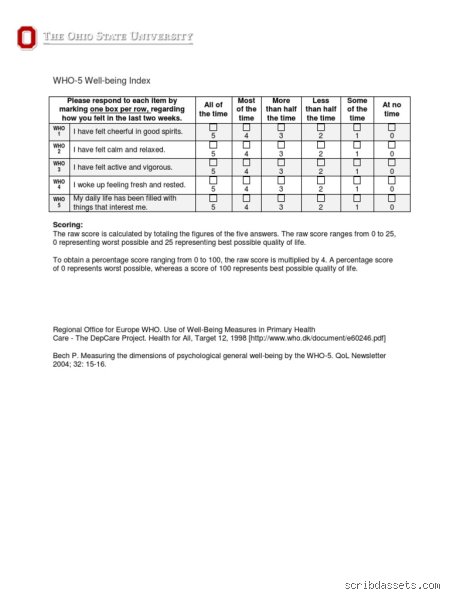
The simplicity is deceptive. Each of the five items is scored on a 6-point Likert scale, ranging from 0 (at no time) to 5 (all of the time). You end up with a raw score between 0 and 25. To make it a percentage, you multiply by four, giving you a final score from 0 to 100. A score below 50 is the "red flag" for low well-being, while anything under 28 usually suggests clinical depression. In a 2015 systematic review of 213 studies, the WHO-5 assessment showed a sensitivity of 0.86 and a specificity of 0.81 for detecting major depression. That is a staggering level of accuracy for something that fits on a sticky note. Yet, people don't think about this enough: a high score doesn't mean you're "cured" of life's problems; it just means your psychological battery has a decent charge today.
The technical architecture: Why these five specific metrics matter
If you look at the items—cheerfulness, calmness, vigor, rest, and interest—you see a balanced ecosystem of human experience. The first item, "I have felt cheerful and in good spirits," targets the core of emotional regulation. But then the scale pivots. It asks about "vigor," which is a fancy way of saying you have the physical "oomph" to get out of bed and do the work. This is where it gets tricky for people with chronic illnesses like Type 2 diabetes. In studies at the Steno Diabetes Center in Copenhagen, researchers found that physical fatigue often masks as psychological distress. The WHO-5 assessment captures this overlap without forcing a diagnosis down the patient's throat before the blood work even comes back.
Validation across cultures and languages
Translating a psychological tool isn't just about swapping words in a dictionary; it’s about capturing the "vibe" of happiness in different cultures. The WHO-5 assessment has been translated into over 30 languages, from Amharic to Urdu. It works in China just as well as it works in Brazil. Why? Because the concepts of "restful sleep" and "interest in things" are fairly universal human traits. Except that in some cultures, the word "cheerful" carries a social weight it doesn't have in others. Despite these linguistic hurdles, the internal consistency (Cronbach’s alpha) usually sits comfortably above 0.80. This means the questions are all pulling in the same direction, which explains why it is so hard to "cheat" the test by overthinking your answers.
Sensitivity to change in therapeutic settings
Doctors love this tool for "monitoring," which is medical-speak for seeing if the pills or the talk therapy are actually doing anything. If a patient’s score jumps from a 32 to a 48 over a month, that is a statistically significant clinical improvement. And honestly, it's unclear if any other short-form tool can track these micro-shifts as effectively. I believe we rely too much on heavy-duty diagnostic interviews like the SCID-5 when a simple WHO-5 assessment done every two weeks would provide a much clearer "weather map" of a patient's recovery trajectory. It’s the difference between a high-resolution photograph and a time-lapse video; the video tells you where the person is going, not just where they are stuck.
How the WHO-5 assessment compares to the PHQ-9 and GAD-7
The Patient Health Questionnaire (PHQ-9) is the "big brother" of the screening world, but it is a bit of a downer. It asks about "failure," "trouble concentrating," and "thoughts that you would be better off dead." While those are vital questions, they can be incredibly triggering if you're just having a slightly off week. The WHO-5 assessment is the polite cousin. It gets to the same destination—identifying who needs help—but it takes a much more scenic, less traumatic route. As a result: patients are less likely to experience "survey fatigue" or "defensive responding" where they lie to avoid a long conversation with a psychiatrist they don't know yet.
The screening paradox in primary care
There is a persistent myth that more questions equal more truth. We're far from it. In fact, adding more items often introduces "noise" into the data. When a GP in a busy London clinic has twelve minutes to see a patient, every second of paperwork is a second taken away from looking the patient in the eye. The WHO-5 assessment takes roughly 45 seconds to complete. This efficiency is the issue remains for many critics who think it's too "lite." But the data suggests otherwise. Because it is so quick, it actually gets used. A long, "better" test that stays in the desk drawer because it's too long is, for all intents and purposes, a useless test. Hence, the brevity is its greatest scientific strength, not a weakness.
Identifying the "Floor Effect" in psychiatric tools
A common problem with mental health scales is the "floor effect," where everyone who isn't clinically depressed scores the same "zero." This makes it impossible to tell a happy person from a very happy person. The WHO-5 assessment avoids this. Because it measures well-being, it can distinguish between someone who is "okay" and someone who is "flourishing." This makes it an excellent tool for positive psychology interventions. If you're running a mindfulness workshop, you don't want to know if people are "less depressed"; you want to know if they are more alive. But let's be real—experts disagree on whether a high well-being score truly negates the presence of underlying anxiety disorders. It is a snapshot of the sun, but it doesn't always tell you if there are storm clouds just beyond the horizon.
Pitfalls and the pervasive fog of misinterpretation
The problem is that the WHO-5 assessment looks deceptively simple, leading practitioners into a trap of casual overconfidence. Many mistakenly treat it as a diagnostic sledgehammer for major depressive disorder. It is not. While it boasts a sensitivity of approximately 0.86 in primary care settings, it remains a screening sieve, not a final verdict. If you see a low score, do not reach for the prescription pad immediately. You must distinguish between clinical depression and transient situational distress. Context matters.
The raw score vs. the percentage scale
Because the raw values range from 0 to 25, novice users often forget the conversion factor. A raw score of 12 does not mean twelve percent; it means forty-eight percent. This mathematical hopscotch creates massive documentation errors in electronic health records. Let's be clear: standardization is the only defense against clinical noise. If the patient scores below 13, or if they answer 0 or 1 on any single item, further investigation becomes mandatory. High specificity is great, yet it vanishes when the math is botched. It happens more often than we care to admit.
Cultural nuances and the language of well-being
Is "feeling cheerful" a universal metric for health? Probably not. The WHO-5 assessment relies on subjective well-being, which is a concept that shifts shape across borders. In certain collectivist cultures, internal emotional states are secondary to social harmony. Using a literal translation without cultural validation renders the data meaningless. We assume everyone understands "vigorous," but to an elderly patient with chronic fatigue, that word is a cruel joke. (Precision in language is often the first casualty of rapid screening).
The temporal shadow: A neglected expert strategy
Most clinicians use the tool as a static snapshot. This is a mistake. The real power of the Well-being Index lies in its longitudinal sensitivity, specifically its ability to track Minimum Clinically Important Difference (MCID). A shift of 10 percent is the threshold. If your patient moves from a 40 to a 50 over three weeks, the intervention is working. But what if they move from 50 to 48? That is just statistical jitter. The issue remains that we ignore the slope of the line in favor of the point on the graph.
The sensitivity to pharmacological change
Research indicates the WHO-5 assessment is more sensitive to the early signs of treatment response than the PHQ-9. Why? Because it measures the presence of the positive rather than just the absence of the negative. In trials involving Type 2 diabetes patients, improvements in well-being often preceded improvements in glycemic control. This suggests that the index serves as a lead indicator for physical health outcomes. And who wouldn't want a crystal ball for metabolic recovery? We should be using this as a weekly pulse check, not a quarterly formality.
Frequently Asked Questions
What is the specific cutoff for a positive screen?
A raw score of less than 13 is the universally accepted clinical threshold for potential depression. Data from large-scale European surveys show that this specific cutoff provides a sensitivity of 0.92 and a specificity of 0.81 for identifying Major Depressive Disorder. As a result: any patient falling below this line requires a follow-up diagnostic interview like the SCID or M.I.D.A.S. to confirm a diagnosis. You must also calculate the percentage score by multiplying the raw sum by four to align with international reporting standards.
Can this index be used for children and adolescents?
The WHO-5 assessment has been validated for use in populations as young as nine years old with high reliability. Which explains why school psychologists are increasingly adopting it over longer, more intrusive behavioral checklists. Studies in pediatric endocrinology have utilized it to monitor the mental health of teenagers managing chronic conditions. It is brief enough to prevent survey fatigue, which is the primary cause of garbage data in youth samples. It works because it respects their limited attention spans.
Does the tool account for physical symptoms of illness?
No, and that is its greatest architectural strength. By focusing exclusively on hedonic and eudaemonic well-being, the 1998 version avoids the "somatic trap" where physical pain is confused with psychological despair. In populations with oncological or cardiovascular diseases, traditional tools often over-diagnose depression because they ask about sleep or appetite. The WHO-5 avoids this entirely. It asks about spirit and interest. This ensures that a patient with chronic insomnia is not mistakenly labeled as depressed simply because they cannot sleep.
The verdict on emotional measurement
We are obsessed with measuring the broken parts of the human psyche while ignoring the vitality that remains. The WHO-5 assessment is a radical act of clinical rebellion because it dares to ask if a person is "awake" to their life. It is not enough to be "not sad"; we must strive for the presence of psychological flourishing. Our healthcare systems are designed to fix leaks, but this tool asks if there is any water in the tank to begin with. In short, if you aren't measuring well-being, you aren't practicing medicine; you are just performing maintenance on a biological machine. Use the scale. Respect the math. Listen to the silence between the scores.