Understanding the ticking plumbing: Why some arteries balloon while others hold firm
An aneurysm isn't some mysterious tumor or a sudden infection; it is quite literally a mechanical failure of the pipe wall. Think of a garden hose with a weak spot that starts to bubble outward under pressure. In the human body, specifically within the Circle of Willis at the base of the brain or the abdominal aorta, the constant thumping of systolic pressure can wear down the tunica media. This is the muscular middle layer of the artery. Once that integrity vanishes, the vessel wall thins out until it is stretched as translucent as a cheap balloon. The thing is, most people walking around with one have absolutely no clue because a "silent" aneurysm rarely pushes on nerves or causes pain until the moment it fails.
The structural anatomy of a blowout
Why do they happen? Doctors point to a messy cocktail of genetics, long-term hypertension, and the lifestyle choices we all know we should avoid. But it gets tricky when you look at the hemodynamics. Blood doesn't just flow; it swirls and eddies at the bifurcations—the forks in the road—of your arteries. If you have a specific genetic predisposition where your collagen synthesis is slightly off, those bifurcations become ground zero for saccular aneurysms. These berry-shaped protrusions account for nearly 90 percent of intracranial cases. Because the wall is lacking a proper internal elastic lamina, it can no longer snap back. It just grows. And grows. Until it doesn't.
The role of flow and friction
We often ignore the sheer violence of our own internal pressure. Imagine 5 liters of blood being forced through a closed loop every sixty seconds, day after day, for seventy years. Yet, some people have massive 15mm bulges that never pop, while others suffer a rupture from a tiny 3mm "baby" aneurysm. This discrepancy drives researchers crazy. (Honestly, it is unclear why some small ones are so much more lethal than their giant cousins). We suspect it has to do with the aspect ratio—the depth of the dome compared to the neck of the aneurysm—which dictates how much turbulent blood gets trapped inside the sac, scouring the weakened wall like sandpaper.
The high-stakes gamble of elective intervention and preventive repair
Deciding to go under the knife when you feel perfectly fine is a psychological nightmare. But when a CTA (Computed Tomography Angiography) reveals a 7mm bulge in your internal carotid artery, the math shifts. The annual risk of rupture for a small, asymptomatic aneurysm is often cited at around 1 percent. That sounds low, right? Except that over twenty years, that cumulative risk becomes a 20 percent chance of a sudden, likely fatal event. That changes everything. I believe we have moved past the era of "watchful waiting" for most healthy patients, as the technology for repair has outpaced the safety of doing nothing.
Surgical clipping: The gold standard of the old guard
Back in 1937, Walter Dandy placed the first silver clip across the neck of an aneurysm, and surprisingly, the basic premise hasn't changed that much. A neurosurgeon performs a craniotomy, peeling back a section of the skull to reach the brain's cisterns. They find the neck of the "berry" and snap a tiny titanium clip onto it. This immediately cuts off the blood flow, essentially "killing" the aneurysm while leaving the main artery intact. It is brutal, invasive, and requires weeks of recovery. Yet, the durability is unmatched; once a clip is on, that aneurysm is effectively gone for life. But is opening the skull always the right move? Experts disagree, especially when the location is deep within the brainstem or the patient is over seventy.
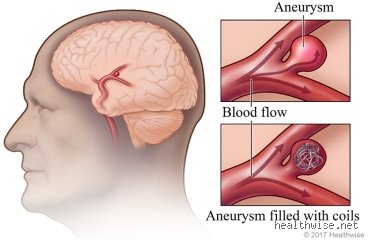
Endovascular coiling: The minimalist revolution
The 1990s brought us the Guglielmi Detachable Coil, and suddenly, the game changed. Instead of a massive incision, a surgeon threads a microcatheter through the femoral artery in your groin all the way up into the brain—a journey of nearly four feet. They pack the aneurysm with hair-thin platinum wires. These coils cause the blood inside the sac to clot, creating a thrombus that seals it off from the inside. It’s elegant. It’s fast. Most patients go home in two days. Because there is no brain retraction involved, the cognitive "fog" associated with traditional surgery is almost non-existent. As a result: the medical community has pivoted hard toward this "inside-out" approach, though it requires more frequent follow-up scans to ensure the coils haven't compressed over time.
Sifting through the data: When is an aneurysm a ticking time bomb?
Not every bulge needs a fix, and that is where the PHASES score comes into play. This clinical tool looks at your age, blood pressure, the size of the aneurysm, and whether you are Japanese or Finnish (who, for reasons involving specific alleles, have much higher rupture rates). A 4mm aneurysm in a 50-year-old smoker with hypertension is a much bigger problem than an 8mm one in an 85-year-old. We're far from a perfect prediction model, but we use these data points to justify the risks of general anesthesia and potential stroke during the repair. The issue remains that we are treating the "average" patient, while every individual's arterial wall thickness is a complete mystery until it's actually seen on the table.
The 7-millimeter threshold controversy
For a long time, 7mm was the magic number. If it was smaller, we left it alone; if it was larger, we operated. But recent studies have shown that 30 to 40 percent of ruptured aneurysms were actually smaller than that threshold when they blew. This realization has sent shockwaves through neurology departments. It suggests that size is a lazy metric. We should be looking at wall shear stress and inflammatory markers instead. If a patient comes in with a "sentinel headache"—a localized, warning-shot pain that precedes a full rupture—size no longer matters. You fix it immediately. Because once that wall lets go, the mortality rate jumps to a horrifying 50 percent within the first few minutes.
Imaging breakthroughs and the 3D advantage
We used to rely on grainy 2D images that looked like Rorschach tests. Now, 3D Rotational Angiography allows surgeons to spin a virtual model of the patient’s vasculature on a screen, spotting "daughter sacs" or irregular blebs that indicate a high risk of imminent failure. These tiny bumps on the main aneurysm are like weak spots on a tire; they are the most likely points of rupture. In 2024, specialized software can even simulate blood flow patterns to predict where the pressure is highest. This level of precision was science fiction twenty years ago. And yet, even with the best maps, the territory remains dangerous because the brain is the most unforgiving workplace in the world.
The hidden risks of "fixing" a problem you didn't know you had
There is a dark side to preventive medicine that people don't think about this enough: the "incidentaloma" trap. With the rise of full-body scans and high-resolution MRIs for minor concussions, we are finding more aneurysms than ever before. This creates a massive psychological burden. Is it better to live in blissful ignorance or to live with the knowledge that a vessel in your head might pop? The International Study of Unruptured Intracranial Aneurysms (ISUIA) sparked massive debate by suggesting that many small aneurysms have a near-zero chance of ever rupturing. This implies we might be over-treating—subjecting people to the 1-2 percent risk of surgical complications for a "disease" that might have never harmed them.
The financial and emotional cost of prevention
A preventive coiling procedure can cost anywhere from $50,000 to $150,000 depending on the hospital and the complexity of the stent-assisted coiling required. Insurance companies hate the ambiguity. But compared to the $500,000+ cost of treating a ruptured patient in the ICU for three weeks, prevention is a bargain. Beyond the money, the emotional toll of "brain surgery" is staggering. I’ve seen patients develop PTSD just from the diagnosis. They stop exercising, they stop having sex, and they live in constant fear of their own pulse. Paradoxically, the stress of knowing you have an aneurysm can raise your blood pressure enough to actually cause the rupture you're so afraid of.
Common blunders and lethal myths
People often imagine a ticking time bomb nestled in the brain or aorta as a loud, rhythmic countdown that anyone could hear if they simply listened closely enough. The reality is far more silent and far more treacherous. One of the most pervasive misconceptions involves the belief that symptomatic warnings always precede a disaster. They do not. Because the vast majority of these vascular dilations remain asymptomatic until the very moment they fail, waiting for a headache or back pain is a gamble with impossible odds. You might feel fine right up until the point you are not. Let's be clear: feeling healthy is not a diagnostic tool for vascular integrity.
The size obsession trap
Clinicians frequently encounter patients who believe a small bulge is a safe bulge. While it is true that an abdominal aortic aneurysm (AAA) is generally monitored until it hits the 5.0 to 5.5 centimeter threshold, size is not the only metric of destruction. A 4-centimeter bulge in a patient with uncontrolled hypertension or a heavy smoking history carries a much higher risk profile than the raw numbers suggest. Wall tension and morphology matter just as much as diameter. The issue remains that we often treat these like balloons, yet human tissue is far more unpredictable than latex. If you ignore a 4.5 cm bulge because it has not hit the magic number yet, you are ignoring the physics of hemodynamic stress that could cause a rupture at any moment.
Misunderstanding the screening process
Another common mistake is the assumption that a standard physical exam will catch every looming threat. Can you fix an aneurysm before it ruptures if your doctor cannot even feel it? Probably not. Statistics from the Society for Vascular Surgery indicate that physical exams only detect about 38 percent of AAA cases in asymptomatic patients. This efficacy drops even lower if the patient has a high Body Mass Index. Relying on a quick poke of the abdomen during an annual checkup is practically useless for detection. Instead, we rely on ultrasound and CT angiography, which offer a 95 to 100 percent sensitivity rate for identifying these silent killers before they turn fatal.
The forgotten factor: The role of biomechanical mapping
While surgeons traditionally look at the widen