The Silent Colonizers: Identifying the Parasite That Attacks the Pancreas
We like to think of our digestive enzymes as an impenetrable chemical barrier. It is a comforting fiction. In reality, certain highly evolved trematodes view the human biliary system as a luxury estate. Clonorchis sinensis is a flatworm that structural biologists marvel at, even as epidemiologists weep over its devastation. It affects over 15 million people globally, heavily concentrated across Russia, China, and Vietnam. But the thing is, global food supply chains mean a plate of undercooked freshwater fish in Chicago could introduce the same pathogen. How does a worm smaller than a fingernail breach an organ designed to digest meat? It crawls. Up the Ampulla of Vater, defying the downward torrent of pancreatic juices.
The Anatomy of an Intrusive Migration
The journey is purely mechanical yet chemically brilliant. Once inside the duodenum, the metacercariae shed their cysts. Most head straight for the common bile duct, but the pancreatic duct is right there, sharing the same anatomical doorway. When a rogue fluke chooses the pancreatic route, it anchors itself using oral suckers. It feeds on the epithelial lining. Because the pancreatic duct in an adult human measures a measly 2 to 4 millimeters in diameter, a single adult fluke measuring 10 to 25 millimeters long causes instant, catastrophic plumbing issues. Think of it like a rag stuffed down a narrow drainpipe; the fluid has nowhere to go but backward.
Pathological Chaos: How Trematodes Disrupt Pancreatic Homeostasis
This is where it gets tricky for the immune system. The pancreas cannot tolerate stagnation. When Clonorchis sinensis or its cousin Opisthorchis viverrini blocks the flow, premature activation of zymogens occurs. Instead of digesting your lunch in the intestine, trypsin and chymotrypsin begin digesting your pancreas. This localized auto-digestion triggers acute pancreatitis. But what happens when the infestation becomes a chronic, decades-long residency? That changes everything. The constant mechanical abrasion from the parasite's scales combined with its toxic excretory-secretory products leads to adenomatous hyperplasia of the ductal epithelium. The tissue scars, narrows, and deforms permanently.
The Carcinogenic Timeline and Radical Nuance
Medical textbooks love a neat narrative linking these parasites exclusively to cholangiocarcinoma, which is cancer of the bile ducts. But honestly, it's unclear why we ignore the secondary pancreatic oncogenesis so aggressively. I argue that the chronic inflammation induced by these flukes is equally capable of driving pancreatic ductal adenocarcinoma. The International Agency for Research on Cancer classified Opisthorchis viverrini as a Group 1 carcinogen back in 1994. Yet, mention a parasite during a pancreatic tumor board meeting in Western Europe, and you will be met with blank stares. We are far from a unified diagnostic consensus here, mostly because Western medicine views helminthiasis as a dead relic of the nineteenth century.
The Nematode Threat: Large-Scale Structural Destruction
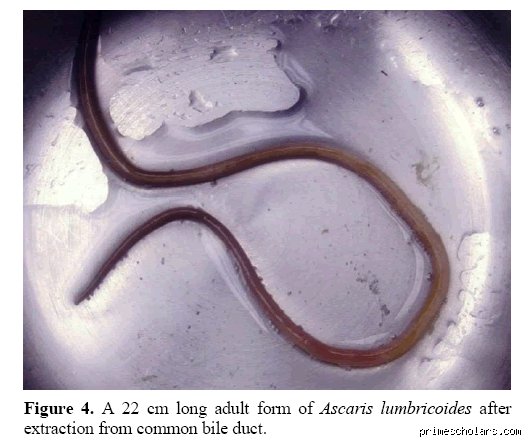
If flukes are subtle saboteurs, Ascaris lumbricoides is a wrecking ball. This giant roundworm, which can grow up to 35 centimeters in length, behaves entirely differently from the flat trematodes. It does not want to live in your pancreas; it gets lost. Ascaris is remarkably hyperactive. Driven by an innate urge to explore narrow orifices, an adult worm roaming the duodenum will probe the opening of the pancreatic duct. It forces its way inside. Can you imagine a muscular, spaghetti-sized worm thrashing around inside a tube the width of a matchstick? The physical pressure alone causes immediate, excruciating biliary colic and necrotizing pancreatitis.
The 2012 Kashmir Study and Clinical Reality
This is not a theoretical nightmare. A seminal study published in India analyzed pancreaticobiliary ascariasis cases in the Kashmir Valley, a major endemic hotspot. Researchers documented that upward of 23 percent of biliary complications in the region stemmed directly from Ascaris migration. The worm enters, dies, and calcifies if left untreated. This calcified corpse becomes the perfect nidus for recurrent stone formation. It is a brutal sequence: mechanical blockage, bacterial infection via transported intestinal E. coli, and eventual tissue necrosis. The issue remains that unless an ultrasound technician specifically looks for the characteristic 'double-tube' sign of a moving worm, the patient ends up on an operating table for standard gallstone removal.
Diagnostic Blindspots: Why Conventional Testing Fails
Why do these infections go unnoticed until the damage is irreversible? People don't think about this enough: our standard diagnostic machinery is calibrated for chemical imbalances and lifestyle diseases, not zoology. A routine serum amylase or lipase test will confirm that the pancreas is inflamed, yes, but it says absolutely nothing about the guest list. Even sophisticated triple-phase CT scans frequently misinterpret a cluster of flukes or an Ascaris remnant as an intraductal papillary mucinous neoplasm or a common cholesterol stone. Which explains why so many patients undergo unnecessary, highly invasive Whipple procedures or partial pancreatectomies when a simple course of antiparasitic medication could have sufficed.
The Limits of O&P Exams and the Serological Alternative
Relying on a standard Ova and Parasite stool exam is a gamble with terrible odds. Flukes shed eggs intermittently. If the pancreatic duct is completely obstructed, those eggs cannot even reach the intestine to be excreted! Hence, a patient can have a pancreas literally teeming with helminths while their stool samples come back pristinely negative three times in a row. As a result, we must pivot toward enzyme-linked immunosorbent assays (ELISA) and polymerase chain reaction (PCR) assays targeting parasitic DNA in duodenal aspirates. Experts disagree on the cost-effectiveness of screening immigrant or traveler populations this way, but when the alternative is pancreatic failure, the hesitation seems absurd.
The Great Mirage: Common Misconceptions Regarding Pancreatic Invaders
Medical folklore frequently misleads the public into believing that global parasitic threats only menace the intestines. The problem is that organisms like Clonorchis sinensis and Opisthorchis viverrini do not read human anatomy textbooks. They migrate. Why do so many patients assume a simple stool test catches everything? Because standard diagnostics frequently miss the stealthy migration of these flukes into the biliary tree and neighboring tissues. A negative stool sample provides false comfort while the true parasite that attacks the pancreas continues its slow, destructive feast upstream.
The Myth of the Bulletproof Western Diet
Many individuals operating under a cloud of geographic arrogance believe raw fish hazards belong exclusively to specific Asian river basins. Except that globalized food supply chains have completely rewritten the rules of epidemiology. If you consume imported, undercooked freshwater fish in a high-end European or American restaurant, you are vulnerable. Statistics from global health registries show that over 35 million people worldwide harbor foodborne trematodes. It is a massive underestimate. Believing your local postal code protects your digestive organs from a parasite that attacks the pancreas is a dangerous, obsolete fantasy.
Antibiotics: The Useless Defense Shield
Let's be clear about pharmaceutical interventions. When sudden, unexplained epigastric agony strikes, panicked individuals often demand broad-spectrum antibiotics from hurried clinicians. But single-celled protozoa or complex multicellular helminths laugh at amoxicillin. Pumping your body full of antibacterial agents merely destroys your beneficial microbiome, which explains why the actual parasitic infection often worsens post-treatment. Targeting a pancreatic fluke requires highly specific anthelmintic agents like praziquantel, administered at precise dosages of 75 mg/kg per day, rather than random, shotgun-approach prescriptions.
The Echo Chamber: A Critical Hidden Dimension
Beyond the mechanical obstruction of ducts, an insidious biochemical warfare transpires within the host. The parasite that attacks the pancreas does not merely occupy physical space; it actively secretes immunomodulatory molecules. These excretory-secretory products alter local cellular behavior, triggering a state of perpetual, low-grade tissue remodeling. Over decades, this silent molecular skirmish transforms healthy glandular tissue into a scarred, fibrotic wasteland, a grim reality that standard abdominal ultrasounds usually fail to capture until structural damage becomes irreversible.
The Malignant Transformation Connection
Can a simple fluke turn tissue carcinogenic? The International Agency for Research on Cancer categorizes specific fish flukes as Group 1 definitive carcinogens. While most research highlights cholangiocarcinoma, the proximity of the pancreatic duct means that chronic, parasite-induced inflammation spills over, dramatically elevating the risk of pancreatic adenocarcinoma. This is not alarmist speculation. Epigenetic alterations induced by the chronic presence of these organisms can mutate cellular DNA. It is a terrifying prospect, yet mainstream clinical screenings for pancreatic oncogenesis regularly ignore parasitic serology altogether.
Frequently Asked Questions
Can a standard routine blood panel detect the parasite that attacks the pancreas?
A basic complete blood count offers mere breadcrumbs rather than a definitive diagnostic smoking gun. While a physician might notice elevated levels of eosinophils—a specific type of white blood cell that surges during helminthic wars—this marker is notoriously fickle and non-specific. Data indicates that fewer than 40% of chronic fluke patients exhibit pronounced peripheral eosinophilia during the latent stages of infection. Consequently, relying on a standard metabolic panel or basic blood count will inevitably leave you stranded in diagnostic limbo. Advanced molecular testing, specifically serum enzyme-linked immunosorbent assays or specialized real-time polymerase chain reaction tests, remains mandatory to unmask the hidden pathogen definitively.
How exactly does a fluke travel from the stomach to the pancreatic duct?
The journey of the juvenile fluke is a masterclass in biological navigation and predatory efficiency. After a human ingests contaminated, metacercariae-laden raw fish, the protective cysts rupture inside the duodenum due to gastric acid exposure. The young parasites do not wander aimlessly; instead, they actively seek the ampulla of Vater, which is the tiny common opening where both bile and pancreatic secretions enter the intestine. Crawling backward against the continuous, downward chemical current, these resilient organisms ascend into the common bile duct and frequently take a wrong turn—or a deliberate detour—directly into the pancreatic conduit. As a result: the delicate tissues of your primary metabolic organ become the final, catastrophic destination for these uninvited biological hitchhikers.
What are the definitive long-term consequences of leaving this infestation untreated?
Ignoring a persistent parasitic colonization within the hepatopancreatic system eventually invites metabolic collapse and structural ruin. Over a period stretching from five to twenty years, the constant mechanical irritation and chemical secretions produce severe chronic pancreatitis. This progressive destruction forces a catastrophic decline in the organ's endocrine and exocrine functions, meaning your body stops producing adequate digestive enzymes and vital regulatory hormones. Clinical studies track a direct, measurable trajectory where up to 15% of chronically infested individuals eventually develop secondary, insulin-dependent diabetes mellitus due to islet cell destruction. In short, a failure to aggressively eradicate the parasite that attacks the pancreas guarantees a future defined by severe nutritional malabsorption, permanent organ scarring, and systemic metabolic dysfunction.
A Radical Shift in Gastrointestinal Vigilance
We must stop treating parasitic diagnostics as an exotic, historical footnote reserved exclusively for tropical medicine textbooks. The modern medical establishment remains dangerously complacent, hiding behind a comfortable shield of conventional imaging while patients suffer from misdiagnosed, chronic abdominal agony. Our globalized food networks require an equally globalized diagnostic mindset. It is time to aggressively mandate specialized serological testing whenever ambiguous pancreatic inflammation presents itself in clinics. Refusing to adapt our diagnostic protocols to the realities of modern culinary transit is nothing short of clinical negligence. We cannot afford to let patients pay the ultimate price with their lives simply because we chose to ignore the microscopic killers hiding in plain sight on our dinner plates.