Beyond the textbook: Understanding the physiological chaos behind the what are the 2 3 criteria for pancreatitis
The pancreas is a moody organ, tucked away behind the stomach, pulling double duty as an endocrine and exocrine powerhouse. When things go south, they go south fast. People often assume that any stomach ache in the upper abdomen might be the culprit, but the pathophysiology of enzyme activation suggests something far more violent is happening internally. I’ve seen cases where the patient describes the pain as a "boring" sensation, not because it is dull, but because it feels like a physical drill is moving through their spine. This isn't your run-of-the-mill indigestion. Because the organ is retroperitoneal, the inflammation irritates the posterior nerves, which explains why leaning forward sometimes offers a tiny, pathetic shred of relief. But why do we use these specific markers? The issue remains that the pancreas is fragile; once the trypsinogen converts to trypsin prematurely inside the acinar cells rather than the duodenum, the chemical fire starts spreading.
The internal combustion of the acinar cells
Most folks don't think about this enough, but the pancreas is basically a bag of grenades with the pins half-pulled. Under normal conditions, these digestive enzymes are kept in an inactive state—proenzymes—until they reach the small intestine. Yet, when a gallstone gets stuck in the Ampulla of Vater or alcohol metabolites reach toxic levels, the system glitches. This intracellular activation leads to autodigestion. The 2 3 criteria for pancreatitis exist because we need a high-specificity net to catch this process before systemic inflammatory response syndrome (SIRS) sets in. It is a race against a biological clock that doesn't care about your weekend plans. And honestly, it’s unclear why some people can drink like a fish for decades with no issues, while others trigger a necrotizing event after one heavy night; the genetic predisposition via the SPINK1 or PRSS1 mutations might be the hidden variable here.
The first pillar: Clinical presentation and the unmistakable nature of pancreatic pain
If you walk into an ER and you aren't doubled over, the triage nurse might not immediately jump to the 2 3 criteria for pancreatitis. The pain is the hallmark. It is sudden. It is unrelenting. We're far from a mild cramp here; we are talking about a VAS score of 9 or 10 in almost every legitimate case. Interestingly, the pain usually reaches its maximum intensity within thirty minutes to an hour. Does it always radiate to the back? No, but in about 50% of cases, that classic "band-like" distribution is present. This is where it gets tricky for doctors—many other conditions like a perforated peptic ulcer or acute cholecystitis can mimic this. Yet, the persistence of the discomfort is what sets it apart. While a gallbladder attack might subside after a few hours of misery, pancreatitis is the guest that refuses to leave, often lasting for days regardless of position or over-the-counter meds.
When the "classic" symptoms decide to go rogue
But here is a sharp opinion that contradicts the standard med-school flowcharts: we rely too much on the "typical" pain profile. In elderly patients or those with long-standing diabetes, the nerve response can be blunted, leading to what some call "painless pancreatitis," though that is a bit of a misnomer. They might just feel profoundly weak or nauseated. Nausea and vomiting occur in about 90% of patients, yet these are so non-specific they are almost useless for a hard diagnosis on their own. As a result: we have to lean heavily on the other two criteria when the clinical picture is blurry. It’s a bit ironic that the most "obvious" symptom is often the one that leads to the most misdiagnoses in the first few hours of a hospital visit. (And let's not even get started on how referred pain in the left shoulder—Kehr’s sign—can occasionally throw a wrench in the works during a physical exam).
The second pillar: The chemical evidence in the bloodstream
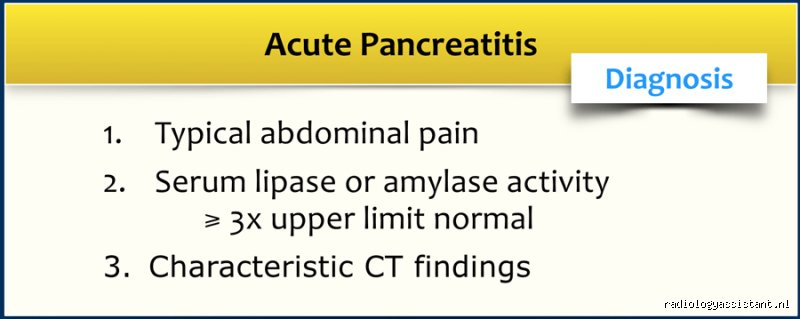
The blood doesn't lie, except when it does. When we look at what are the 2 3 criteria for pancreatitis, the biochemical markers are the heavy hitters. We are looking for serum lipase or serum amylase levels to be at least 3x the normal limit (usually meaning over 160 U/L for lipase, depending on the lab's specific equipment). Lipase is the golden child here. It stays elevated longer—up to 8 to 14 days—making it much more reliable than amylase, which can drop back to normal within 48 hours. If a patient waits three days to go to the doctor because they thought it was just "bad shrimp," the amylase might already be back to baseline. That changes everything. That is why most modern protocols have essentially demoted amylase to a secondary role, even though it’s still technically part of the official triad.
Lipase versus Amylase: The battle for diagnostic supremacy
Why do we still talk about amylase at all? It's cheap, it's fast, and in hypertriglyceridemia-induced pancreatitis, amylase might actually be falsely low, which is a terrifying prospect if you aren't looking for it. In these cases, the excess fat in the blood interferes with the lab's colorimetric assays. Which explains why a savvy doctor will look at the serum triglyceride levels—if they are over 1000 mg/dL, the 2 3 criteria for pancreatitis might be met even if the enzymes look weirdly subdued. But for the vast majority, the lipase elevation is the smoking gun. It is produced almost exclusively by the pancreas, whereas amylase is also churned out by your salivary glands (hello, mumps) and even your fallopian tubes. You don't want a diagnosis based on a saliva leak when your pancreas is the one screaming for help.
The third pillar: Imaging and the visual confirmation of a "misty" mesentery
You’d think we would scan everyone immediately, but the thing is, early imaging is often a waste of time and money. If the first two criteria are met, a contrast-enhanced CT (CECT) doesn't actually change the initial treatment—which is mostly just aggressive fluids and fasting. In fact, if you scan someone within the first 24 hours, the pancreas might look perfectly normal. The peripancreatic inflammatory changes and fat stranding take time to develop. However, imaging becomes paramount—wait, scratch that—imaging becomes the decider when the bloodwork is ambiguous. We look for focal or diffuse enlargement of the gland. On a CT scan, a healthy pancreas has crisp edges; an inflamed one looks shaggy, blurred, or "misty" as the fluid starts to leak into the surrounding tissue.
CT, MRI, or Ultrasound: Choosing the right lens
The choice of tool matters immensely. An abdominal ultrasound is usually the first thing ordered, not to see the pancreas (which is often obscured by bowel gas—thanks, biology), but to look for gallstones. If the common bile duct is dilated beyond 6mm, we’ve likely found our culprit. But if we suspect necrotizing pancreatitis, we need the big guns. A CT with IV contrast is the gold standard for spotting non-enhancing parenchyma, which is just a fancy way of saying "dead tissue." This usually isn't visible until 48 to 72 hours after the pain starts. Experts disagree on exactly when to pull the trigger on a scan, but the general consensus is to wait unless the patient is crashing. In short, the 2 3 criteria for pancreatitis allow for a diagnosis without a single radiation dose, provided the symptoms and the labs align like stars in a very painful galaxy.
Misdiagnoses and the pitfalls of clinical shortcuts
The problem is that clinicians occasionally treat the Atlanta Criteria like a rigid checkbox rather than a nuanced diagnostic tapestry. You might see a patient doubling over with epigastric pain and instantly reach for the order sheet, yet elevated enzymes do not always equate to a dying pancreas. Let's be clear: a serum lipase level can skyrocket due to renal failure or a perforated peptic ulcer, confusing the unwary practitioner. If you rely solely on numbers, you risk missing the forest for the enzymes.
The trap of the "slightly elevated" lipase
Because the guidelines demand a threefold increase above the upper limit of normal, a level that is merely double the standard threshold remains a diagnostic "no man's land." Practitioners often succumb to premature closure here. They see a lipase of 350 IU/L when the limit is 160 IU/L and start the IV fluids. But this is a mistake. Without the requisite 3:1 ratio, the specificity for acute pancreatitis drops significantly, sometimes falling below 60 percent in various observational cohorts. Is it really worth labeling a patient with a lifelong gastrointestinal red flag based on a mediocre blood draw? Probably not.
Imaging impatience and the timing blunder
Speed is rarely your friend when it comes to the CT scan. The issue remains that pancreatic necrosis—the literal death of the organ tissue—takes time to manifest on a contrast-enhanced image. Ordering a scan within the first 12 hours of symptom onset frequently yields a "normal" result, providing a dangerous false sense of security. As a result: many patients are discharged only to return with walled-off collections or systemic inflammatory response syndrome (SIRS) two days later. Waiting 48 to 72 hours for that definitive "third criterion" isn't being lazy; it is being methodical.
The hidden impact of the gut-lung axis
Expert management transcends the mere identification of what are the 2 3 criteria for pancreatitis and moves into the realm of organ crosstalk. We often ignore how the pancreas screams at the lungs. In nearly 15 to 20 percent of severe cases, the real danger is not the abdominal pain but the rapid onset of Acute Respiratory Distress Syndrome (ARDS). The enzymes leaking into the bloodstream act like a chemical scorched-earth policy, damaging the delicate alveolar-capillary membrane. (And yes, your patient can drown in their own fluids while you are still obsessing over their lipase levels.)
The gold standard of early enteral feeding
Conventional wisdom once dictated "NPO" or "nothing by mouth" for days to let the pancreas rest. Yet, modern evidence suggests that keeping the gut moving prevents bacterial translocation from the intestines into the necrotic pancreas. Data shows that starting low-fat enteral nutrition within 24 hours reduces infectious complications by roughly 50 percent compared to total parenteral nutrition. Which explains why we now push for early feeding rather than starving the patient into a secondary infection. It feels counterintuitive to feed someone who is vomiting, but the science is unyielding.
Frequently Asked Questions
Can you have pancreatitis with normal lipase levels?
Statistically, roughly 5 to 10 percent of patients with acute pancreatitis will present with normal or near-normal enzyme levels. This phenomenon is most common in cases of hypertriglyceridemia-induced pancreatitis, where high levels of blood fats interfere with the laboratory assays. In these specific scenarios, the serum may appear milky or lipemic, essentially masking the true enzymatic activity. If the clinical suspicion is high but the blood work is clean, the diagnosis must pivot entirely to cross-sectional imaging to satisfy the requirement of what are the 2 3 criteria for pancreatitis. A CT scan showing peripancreatic stranding becomes the "get out of jail free" card for the diagnosis.
How long do these diagnostic criteria remain valid during an attack?
The window for capturing elevated enzymes is surprisingly narrow, as lipase and amylase usually return to baseline within 3 to 7 days. If a patient waits a week to seek medical attention, your blood tests may provide a false negative result. At that point, the radiological evidence remains the only reliable pillar for confirmation. This is why retrospective diagnosis is so difficult in primary care settings without initial acute-phase data. You must document the onset of pain precisely to interpret the biochemical markers within their proper temporal context.
Does the severity of the pain correlate with the severity of the disease?
Paradoxically, the "10 out of 10" pain a patient describes does not always predict a necrotic or life-threatening outcome. Some patients with mild, edematous pancreatitis experience excruciating agony, while those with massive necrosis might present with dull, vague discomfort. We use scoring systems like the BISAP score or Ranson's criteria to judge prognosis because the patient's subjective pain scale is notoriously unreliable for mapping internal damage. Focusing on the patient's vitals—specifically heart rate and urinary output—provides a much clearer picture of the physiological storm than their verbal pain rating ever will.
Beyond the Checkbox: A Clinical Stance
The obsession with satisfying the technical definitions of what are the 2 3 criteria for pancreatitis has created a generation of "protocol-slaves" who forget to look at the human being in the bed. While the Revised Atlanta Classification provides a sturdy framework, it is not a substitute for aggressive, early resuscitation and vigilant monitoring. I take the position that we spend far too much time debating whether an enzyme level is 2.9 or 3.1 times the limit while ignoring the rising creatinine that signals impending multi-organ failure. Diagnostics are the starting line, not the finish. If you wait for the CT scan to tell you the patient is sick, you have already lost the battle. Real expertise lies in the space between the criteria, where intuition meets evidence-based physiology to prevent a routine inflammation from turning into a fatal cascade. Stop treating the paper and start treating the perfusion.