The Spectrum Shift: Defining Pathological Demand Avoidance in the Modern Era
We need to stop viewing this as a behavioral choice. When a child flips a table because someone asked them to put on their shoes, they aren't being malicious; rather, their nervous system has misidentified a minor request as a life-threatening encounter. Elizabeth Newson first coined the term in 1983 at the University of Nottingham, yet the clinical world is still dragging its feet on a universal definition. The thing is, calling it "pathological" feels inherently flawed and deeply unfair to the kids living it. Is it a disease? No, it is a survival strategy driven by an intense, subterranean need for control.
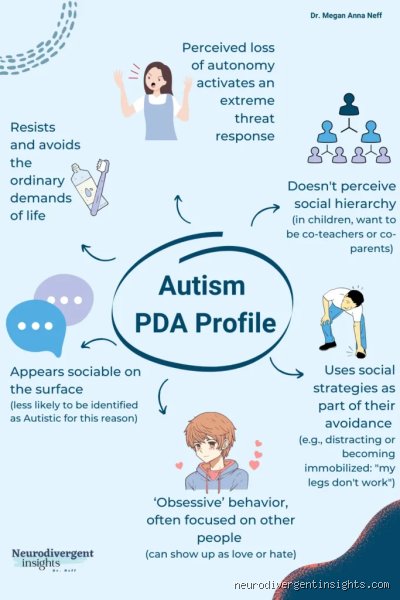
The Core Traits Beyond Simple Refusal
Traditional autism often involves a preference for routine, but PDA flips the script completely. These children use highly social strategies to evade demands, ranging from distraction and negotiation to sudden, overwhelming meltdowns. They might mask their anxiety behind a facade of adult-like competence or use fantasy to escape the crushing weight of expectation. Because their social understanding is often superficial rather than intuitive, they frequently miss the unspoken hierarchy between children and adults, viewing themselves as absolute equals to their teachers or parents.
Why Language Matters in the Diagnosis
Language shapes reality, especially in neurodivergence. Shifting the acronym toward Pervasive Drive for Autonomy redirects the clinical gaze from what the child does wrong to what the child fundamentally needs to survive. The issue remains that standard diagnostic manuals like the DSM-5 still do not officially recognize PDA as a standalone condition, forcing clinicians to categorize it under the broader umbrella of Autism Spectrum Disorder (ASD). This lack of formal recognition means thousands of families go years without answers, trapped in a cycle of inappropriate behavioral interventions that actually make the condition worse.
The Neurological Blueprint: How the Amygdala Hijacks Everyday Requests
Why does a child develop PDA at a biological level? The answer lies deep within the evolutionarily ancient parts of the brain, specifically the amygdala, which acts as the body's smoke detector. In a neurotypical brain, a request like "please brush your teeth" passes through the prefrontal cortex, which weighs the demand and schedules the action. In a PDA brain, that same sentence bypasses logic entirely, triggering an immediate, involuntary flood of adrenaline and cortisol. The child is suddenly in a state of physiological panic.
The Autonomic Nervous System on High Alert
Imagine living in a world where every polite suggestion feels like a loaded gun pointed at your chest. That changes everything about how we view their behavior, doesn't it? Neuroimaging studies, including those reviewed by the National Autistic Society in 2021, suggest structural differences in the pathways connecting the limbic system to the frontal lobes. When a demand is perceived, the sympathetic nervous system takes the wheel. The child cannot help their reaction; they are trapped in a biological feedback loop of fight, flight, or freeze before they can even consciously register what was asked of them.
The Role of Cumulative Cognitive Load
Anxiety is not a static metric. It builds quietly throughout the day, a phenomenon clinicians refer to as vulnerability to demand overload or cumulative toll. A child might tolerate putting on their coat in the morning, tolerate the school bus, and tolerate the morning bell, but by lunchtime, their cognitive reservoir is entirely empty. This explains why a seemingly trivial trigger—like being offered the wrong color cup at 3:00 PM—can cause an explosive meltdown that looks entirely disproportionate to the casual observer. It was never about the cup.
Neurotransmitter Dysregulation and Reward Processing
People don't think about this enough, but the brain's internal reward chemistry behaves differently in these individuals. Dopamine pathways, which typically provide a sense of satisfaction upon completing a task or pleasing an authority figure, do not function the same way in a PDA profile. Traditional praise does not work; in fact, telling a PDA child "good job" often triggers an immediate spike in anxiety because it implies an expectation to repeat the performance. Their neurological architecture is hardwired to resist external reinforcement, seeking safety exclusively through self-directed autonomy.
Genetic Predisposition and Heritability: The Roots of Neurodivergence
No one wakes up one day and decides to have an anxiety-driven need for total control. The etiology of why does a child develop PDA is deeply intertwined with heritable genetic factors, mirroring the broader trends observed across the entire autism spectrum. Epidemiological data from a comprehensive 2019 Swedish twin study demonstrated that autism spectrum traits have a heritability rate of approximately 80% to 90%. PDA does not emerge from a vacuum; it is a specific expression of these highly heritable neural variations.
The Complex Polygenic Architecture
There is no single "PDA gene" that researchers can point to under a microscope. Instead, it is a polygenic phenomenon, meaning it results from the complex, combined influence of hundreds of minor genetic variations acting in concert. These genetic quirks influence everything from synaptic pruning during early childhood development to the density of serotonin receptors in the brain. Where it gets tricky is determining exactly which combination of genes tips the balance from a standard presentation of autism into this highly specific, demand-resistant profile.
Epigenetic Triggers and Early Environment
Genetics loads the gun, but the environment pulls the trigger. Epigenetics refers to how environmental factors can alter the way genes are expressed without changing the underlying DNA sequence. For a child genetically predisposed to this profile, experiencing early medical trauma, chronic sensory overload, or an intensely rigid daycare environment can activate specific genetic pathways. This environmental friction accelerates the development of the intense threat response that characterizes the condition, cementing the PDA profile early in life.
Distinguishing PDA from Oppositional Defiant Disorder: A Critical Diagnostic Boundary
Misdiagnosis is the great tragedy of this condition. Because the outward behaviors look identical to the naked eye—refusal, anger, defiance—untrained clinicians routinely slap these children with a label of Oppositional Defiant Disorder (ODD). But we're far from it when it comes to the actual internal mechanisms driving the behavior. Treating a PDA child with the behavioral modification protocols designed for ODD is a recipe for psychological disaster.
The Motivational Divide Between Control and Compliance
The fundamental difference lies in what motivates the resistance. A child with ODD is typically reacting against authority figures, intentionally testing boundaries, and may find a degree of satisfaction in the conflict itself. Yet, a child with PDA is not fighting the person; they are fighting the demand because it threatens their internal sense of safety. They will avoid demands that they actually want to do—such as playing a favorite video game or eating their favorite food—simply because the activity has been framed as an expectation. ODD kids rarely refuse things they actively enjoy.
The Impact of Traditional Behavioral Interventions
This is where conventional parenting advice completely implodes. Standard behavioral therapy relies heavily on operant conditioning, utilizing strict boundaries, reward charts, and logical consequences to shape behavior. If you try this with a PDA child, their anxiety will skyrocket, leading to complete school refusal, selective mutism, or severe self-harm. They perceive reward charts as a manipulative form of coercion, which drives their threat response even higher. They need collaboration and low-demand lifestyles, not firmer boundaries.
Common mistakes and misdiagnoses in early childhood
The trap of the "defiant" label
Walk into any mainstream classroom and you will witness the standard disciplinary playbook: sticker charts, token economies, and firm boundaries. For a neurotypical child, this structure anchors them. For a child with Pathological Demand Avoidance, these well-intentioned tools act like lighter fluid on an open flame. Traditional behavioral modification assumes the child is choosing to rebel. PDA is a neurological threat-response system, not a behavioral choice. When a teacher tightens the reins, the child's nervous system registers a mortal peril, triggering immediate meltdowns or sudden, terrifying catatonia. We mistake panic for insolence because the trigger looks so mundane to our adult eyes. Why does a child develop PDA traits that mimic oppositional defiance? Because their survival brain cannot differentiate between a tiger in the bushes and a sudden command to put on shoes.
The exhausting mask of the quiet avoider
But let's be clear: the explosive child is only one side of the coin. Clinicians routinely overlook girls who present with internalizing presentations. These children do not scream; instead, they use social mimicry, elaborate excuses, or intense fantasy worlds to evade expectations. A girl might spend seven hours at school looking flawlessly compliant, only to experience a massive, destructive neurological collapse the second she crosses her home threshold. The issue remains that schools misinterpret this compliance as wellness, leaving parents isolated and gaslit by professionals who claim the issue only exists within the home. Research indicates that over 70% of PDA individuals mask their symptoms in public settings, a exhausting feat that takes a massive toll on their mental stability.
The hidden engine of role-equality and expert reframing
Dethroning the traditional adult-child hierarchy
If you want to understand the true core of this presentation, you must look past the avoidance itself and examine the social dynamic. A child navigating this reality operates on an intuitive expectation of absolute role equality. They do not view themselves as a subordinate child to an authority figure, but as an equal peer. Consequently, any top-down command feels like a violent upending of their safety. Can you imagine the sheer terror of being forced into submission by someone you perceive as an equal peer? To de-escalate this, experts advocate for collaborative, low-demand lifestyle frameworks. You must drop the parental imperative and use declarative language instead. Instead of saying, "Get your coat on now," you might say, "The weather forecast says it is freezing outside." This subtle shift gives the child the autonomy to process the information without triggering their threat response.
Frequently Asked Questions
Is Pathological Demand Avoidance officially recognized in major diagnostic manuals?
The global psychiatric community remains divided on its formal categorization, meaning you will not find it listed as a standalone condition in the DSM-5 or the ICD-11. Instead, clinicians diagnose it as a specific behavioral profile under the broader umbrella of Autism Spectrum Disorder. Data from specialized neurodevelopmental clinics in the United Kingdom indicate that approximately 11% of autistic children fit this specific profile, highlighting a significant sub-population within the spectrum. This lack of formal manual recognition creates immense systemic barriers for families seeking educational accommodations. Parents must frequently secure expensive private evaluations to get the necessary school support, which explains why so many children remain mislabeled for years.
Can trauma or poor parenting styles cause a child to develop this condition?
Decades of rigorous genetic and neurological research have thoroughly debunked the toxic myth of the "refrigerator mother" or inadequate discipline causing this profile. PDA is an innate neurodevelopmental configuration that alters how the brain processes environmental demands and social hierarchy from birth. Yet, an invalidating environment or punitive parenting can severely exacerbate the underlying anxiety, transforming a manageable neurological difference into a agonizing mental health crisis. Because the condition is rooted in autonomic nervous system reactivity, traditional harsh discipline actually damages the child's brain development rather than correcting their behavior. We must view it as an innate neurological wiring issue rather than a failure of household rules.
How does this profile differ from standard Oppositional Defiant Disorder?
The distinction lies within the underlying motivation and the consistency of the behavior across different life domains. Children with Oppositional Defiant Disorder usually direct their hostility toward authority figures, whereas a child with this specific profile avoids demands from anyone, including themselves. They will actively avoid things they genuinely want to do, like eating their favorite meal or playing a beloved video game, simply because the desire itself registers as an internal expectation. Statistics reveal that traditional behavioral therapy boasts a success rate below 15% for PDA populations, while it often yields positive outcomes for standard ODD. The issue is fundamentally about anxiety and a desperate need for control, not malice or a desire to dominate others.
The paradigm shift we desperately need
We must stop trying to fix these children and start fixing the environments that break them. Continuing to view this neurotype through the lens of pathology or broken behavior is a collective failure of imagination and empathy. Autistic children with a demand-avoidant profile possess an exquisite sensitivity to control that exposes the inherent flaws in our rigid, compliance-obsessed societal structures. As a result: we must move entirely away from standard behavioral interventions and adopt a radical framework of radical acceptance and shared autonomy. This is not about letting a child rule the household; it is about building a psychological sanctuary where their nervous system can finally step down from red alert. It is time to retire the outdated disciplinary rulebook and build a world where compliance is no longer the metric of a child's worth.