The False Cleanliness Narrative: What Are OCD People Like in the Real World?
Let's be completely honest here. If you ask the average person on the street to describe someone with this diagnosis, they will inevitably conjure up an image of someone washing their hands until they bleed or rearranging books by alphabetical order. But we are far from it. That changes everything when you realize that many individuals with severe symptoms live in what looks like absolute chaos. Their bedrooms might be cluttered, their desks piled high with papers, because the mental energy required to sort things according to their specific, exhausting internal rules is simply too overwhelming to face on a Tuesday morning. The issue remains that the public mistakes a highly specific manifestation of a disorder for its universal definition.
The Hidden Spectrum of Invisible Intrusions
The clinical reality is incredibly vast and frequently terrifying. Where it gets tricky is understanding that the obsession rarely matches the visible behavior in a way that makes sense to an outsider. A person might be paralyzed by the sudden, vivid mental image of steering their car into oncoming traffic—a classic manifestation of Harm OCD—despite being a pacifist who avoids even verbal confrontations. They don't want to do it. The thought disgusts them. Yet, the brain treats this random neurological misfire as an immediate, existential threat. To cope, they might mentally replay their entire morning drive, counting every green light they passed to prove to themselves they are a safe driver. It is a completely silent, invisible torment.
Why Logic Fails to Break the Loop
People don't think about this enough: individuals with this condition usually possess completely intact insight. They know, with absolute intellectual certainty, that checking the front door lock forty-seven times will not change whether it is locked. But the thing is, the emotional center of the brain—the amygdala—is screaming that the house will burn down if they don't turn back. Can you imagine the sheer exhaustion of knowing your actions are irrational while being utterly powerless to stop them? This cognitive dissonance creates a profound sense of shame, which explains why the average delay between symptom onset and proper diagnosis stretches to a heartbreaking nine years.
Inside the Neurobiology: The Broken Braking System of the Mind
To dissect what are OCD people like from a scientific standpoint, we have to look past the psychological distress and peer directly into the cortical-striatal-thalamo-cortical (CSTC) circuit. In a healthy brain, this loop acts as a filter, sorting through millions of random thoughts and discarding the junk data. In a brain affected by this pathology, however, the filter fails. A baseline study conducted at the University of Michigan in 2018 utilized functional MRI technology to demonstrate that patients exhibit severe hyperconnectivity within this circuit. It is as if the brain's braking system has completely failed, leaving the engine revving at maximum capacity over a minor, irrelevant data point.
The Cortical-Striatal-Thalamo-Cortical Circuit Explained
Think of the CSTC circuit as an office bureaucracy where the memo for a false alarm gets stuck on a loop, constantly re-printing itself and demanding immediate action from the CEO. The orbitofrontal cortex detects a potential mistake, the caudate nucleus fails to suppress the signal, and the thalamus keeps the entire system on high alert. As a result: the person experiences a physical sensation of dread that cannot be reasoned away. This isn't a matter of someone being "too sensitive" or needing to "just relax." It is a structural, chemical misfire involving serotonin and glutamate pathways, a biological reality that requires targeted therapeutic intervention rather than well-meaning but useless lifestyle advice.
The Compulsion as a Temporary Safety Valve
When the anxiety reaches an unendurable crescendo, the compulsion steps in as a desperate survival mechanism. It works, too—except that the relief lasts for only a fleeting second. If someone fears contamination, scrubbing their hands provides a sudden drop in cortisol. But this drop acts as a dangerous trap. The brain learns that the ritual "saved" it from danger, reinforcing the neural pathway and ensuring the obsession will return with even greater force tomorrow. It is a cruel psychological extortion racket.
The Multi-Faceted Manifestations: Moving Beyond Germophobia
The clinical presentation changes dramatically from one patient to the next, making standard checklists almost useless. Dr. Jeffrey Schwartz, a research psychiatrist at UCLA who pioneered neuroplasticity-based treatments in the 1990s, categorized these presentations into distinct, often overlapping subtypes. While one individual might spend four hours checking electrical outlets due to a catastrophic fear of fire, another might suffer from scrupulosity—a agonizing form of the disorder focused on moral or religious perfectionism, where a single bad thought is viewed as an unforgivable sin. The external behaviors look totally different, yet the underlying mechanism is identical.
Symmetry, Ordering, and the Need for "Just Right"
For some, the driving force isn't a specific catastrophic fear like illness or death, but rather an intense, abstract discomfort known as the "just right" feeling. They might have to touch a door frame with both elbows until the physical sensation feels perfectly balanced. If the symmetry is disrupted, an overwhelming wave of existential dread washes over them. It resembles a severe itch inside the skull that can only be scratched by executing a precise, arbitrary physical choreography. Experts disagree on the exact evolutionary origin of this specific subtype, but honestly, it's unclear why the human brain attaches such terrifying weight to spatial symmetry.
Relationship OCD and the Cycle of Constant Reassurance
Then there is the relational dimension, an area that receives almost no mainstream media attention. Relationship OCD involves a agonizing, constant questioning of one's feelings toward a partner. Am I truly in love? Are they the one? Is that minor flaw a sign we should break up? To neutralize this panic, the individual might spend hours analyzing past conversations, reading old text messages, or asking friends for reassurance. This constant checking strips away the possibility of intimacy, transforming a loving partnership into a sterile laboratory where every emotion is dissected under a microscope until it dies.
Differential Diagnosis: Distinguishing Genuine OCD from its Imitators
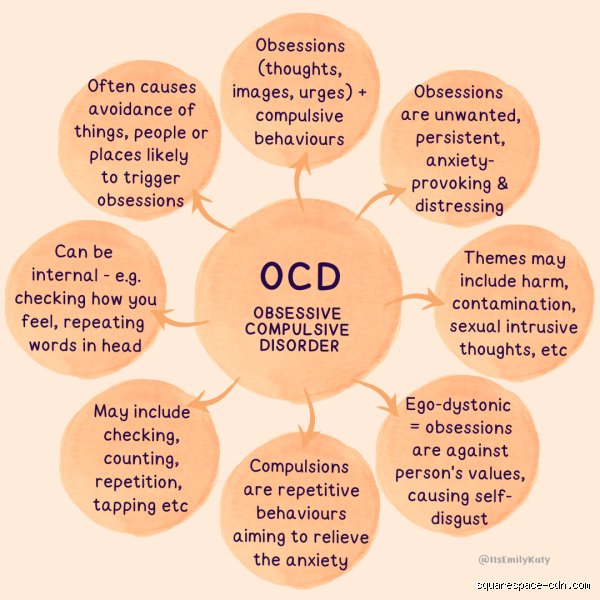
This is where we must draw a sharp, uncompromising line between this debilitating condition and other psychiatric phenomena that look similar on the surface but possess fundamentally different roots. The most common confusion occurs with Obsessive-Compulsive Personality Disorder (OCPD). Despite the overlapping names, these two diagnoses are miles apart. The core distinction lies in how the individual views their symptoms. A person with OCPD is ego-syntonic; they believe their rigid rules, extreme perfectionism, and hoarding behaviors are correct, efficient, and highly desirable. They think the rest of the world is sloppy.
Ego-Dystonic Suffering vs. Ego-Syntonic Pride
Conversely, true Obsessive-Compulsive Disorder is profoundly ego-dystonic. The thoughts and impulses are completely alien to the person's actual values, desires, and self-image. A mother suffering from postpartum intrusions might love her newborn baby unconditionally, yet be tormented by vivid flashes of dropping the infant down the stairs. She hates the thoughts. They cause her immense suffering and guilt. I have seen how this specific distinction determines the entire trajectory of psychiatric treatment, because treating an ego-dystonic intrusion requires an entirely different therapeutic framework than managing an ego-syntonic personality trait.
Anxiety Disorders and General Hypervigilance
But what about generalized anxiety? A person with a severe anxiety disorder worries constantly about real-world issues: finances, health, job security, or global stability. Their mind jumps from one catastrophic scenario to another. For someone with a compulsive diagnosis, the focus narrows down to a highly specific, often bizarre premise that involves a rigid cause-and-effect relationship. They don't just worry about their house burning down; they believe that if they don't tap the coffee maker three times, the house will burn down. The presence of these highly ritualized, specific behavioral defenses is what sets this condition apart from the broad, amorphous cloud of general hypervigilance.
The Mirage of the "Quirky Clean" Persona: Common Misconceptions
Pop culture has reduced a devastating psychiatric condition to a punchline about color-coded highlighters. Let's be clear: clinical obsession is not a personality trait or a synonym for being organized. When society asks what are OCD people like, the collective imagination conjures images of pristine desks and spotless kitchens. The reality is far messier. A person paralyzed by intrusive thoughts might live in absolute chaos because touching a cleaning product triggers a three-hour decontamination ritual they desperately want to avoid.
The Organizing Myth
An obsession is an involuntary, intrusive thought that causes immense distress. A compulsion is the desperate, exhausting behavior performed to neutralize that anxiety. There is nothing neat about it. For instance, an individual might spend forty minutes aligning a single coffee mug to prevent a imagined catastrophe. It looks like perfectionism from the outside, but internally, it is sheer terror. Which explains why people with this diagnosis often feel deeply alienated by the casual misuse of their struggle.
The "We Are All a Little OCD" Fallacy
You like your books arranged alphabetically? That does not mean you share a fraction of this illness. The issue remains a matter of functional impairment and profound suffering. Epidemiological data indicates that true OCD affects roughly 1% to 2% of the global population, a statistic that underscores its status as a distinct, debilitating disorder rather than a universal quirk. Equating normal preferences with a neurobiological condition trivializes the agonizing hours sufferers spend trapped in mental loops. It silences those who genuinely need intervention.
The Hidden Architecture of Mental Compulsions
Most onlookers expect to see visible rituals like handwashing or door-checking. Yet, a massive portion of the battle takes place entirely behind closed eyes. Pure Obsessional OCD, or "Pure O," involves no overt behavioral compulsions at all. Instead, the individual engages in frantic mental gymnastics, seeking reassurance or replaying memories to prove their own safety. Why do we keep looking for external signs when the real destruction occurs within the subconscious?
The Trap of Hyper-Responsibility
What are OCD people like when dealing with uncertainty? They are hyper-vigilant, carrying an inflated sense of personal responsibility for events completely beyond their control. If a tragedy occurs halfway across the world, a sufferer might secretly fear their negative thoughts caused it. This cognitive distortion creates an unbearable psychological burden. As a result: individuals often withdraw from social circles entirely to minimize potential triggers, leading to profound isolation that compounds their depressive symptoms.
Frequently Asked Questions
Is OCD a lifelong condition?
While there is no definitive cure, the disorder is highly manageable with targeted, evidence-based interventions. Longitudinal studies show that roughly 30% to 60% of patients experience significant symptom reduction when treated with Exposure and Response Prevention (ERP) therapy. This behavioral approach forces individuals to confront their triggers without performing the neutralizing compulsion. (It is an incredibly grueling process, to put it mildly.) Medications, specifically Selective Serotonin Reuptake Inhibitors, are also frequently prescribed to help stabilize brain chemistry. In short, while the underlying vulnerability often persists, people can regain complete control over their daily functioning.
At what age do these symptoms typically surface?
The onset of this condition generally follows a bimodal distribution, appearing either in early childhood or during late adolescence. Data from the National Institute of Mental Health confirms the average age of onset is 19 years old, with boys often showing symptoms earlier than girls. Pediatric cases can manifest suddenly, sometimes linked to autoimmune reactions. Because young people frequently hide their rituals out of shame, the lag between symptom onset and professional diagnosis averages an astonishing nine years. Early screening is therefore imperative to prevent the crystallization of these exhausting behavioral loops.
Can stress directly cause someone to develop OCD?
Stress does not create the disorder from scratch, but it acts as a massive accelerant for those with a genetic predisposition. Neuroimaging reveals that sufferers exhibit structural differences in the orbitofrontal cortex and caudate nucleus compared to neurotypical brains. Environmental pressure simply pushes an already vulnerable system over the edge. But a sudden traumatic event can cause mild, manageable tendencies to explode into full-blown, incapacitating compulsions. What are OCD people like during high-stress periods? They are frequently trapped in overdrive, as the brain mistakes abstract doubts for immediate, physical threats to survival.
A Paradigm Shift in Empathy
We must stop treating this neurobiological torment as a quirky preference for tidiness. The ongoing romanticization of mental illness does a profound disservice to those losing hours of their lives to invisible terrors. Except that changing public perception requires more than just polite awareness campaigns; it demands a aggressive dismantling of the stereotypes we consume daily. Sufferers are not tidy perfectionists, nor are they fragile caricatures. They are individuals navigating a glitching neural alarm system with immense resilience. Our collective responsibility is to provide clinical understanding, not trivializing labels that minimize their daily bravery.