Let’s be real for a second: the idea of a surgeon opening your skull to tinker with a blood vessel is terrifying. We often treat neurosurgery with a kind of hushed reverence, as if the technical brilliance of the surgeon somehow negates the messy, unpredictable aftermath for the patient. But here is the thing: the brain is an incredibly sensitive organ that doesn't particularly enjoy being touched, even by the most skilled hands at the Mayo Clinic or Johns Hopkins. When we talk about the side effects of aneurysm clipping, we aren't just discussing a list of symptoms in a textbook; we are talking about a fundamental disruption of the body’s command center. Some people bounce back in weeks, while others find that their short-term memory feels like it’s been through a paper shredder. It’s a gamble, albeit one where the stakes—preventing a catastrophic subarachnoid hemorrhage—usually justify the risk. Yet, the medical community sometimes downplays the "minor" deficits, focusing instead on survival rates. I think that is a mistake because a survivor who can’t recognize their own spouse’s tone of voice hasn't fully "recovered" in any sense that actually matters.
What Actually Happens to the Brain During the Clipping Process?
The Mechanical Reality of the Craniotomy
The journey begins with a craniotomy, a surgical opening of the skull that sounds like something out of a Victorian horror novel but is actually a highly refined procedure. Surgeons must navigate past the protective layers of the brain—the dura mater—to reach the subarachnoid space. This mechanical intrusion is the primary source of early-stage side effects of aneurysm clipping. Because the brain is encased in a rigid container, any inflammation caused by the surgery leads to increased intracranial pressure. Imagine your brain trying to swell inside a stone box. That pressure manifests as intense, pounding headaches that can last for weeks, often requiring a cocktail of steroids and analgesics to manage. It’s not just pain; it’s the sensation of the brain resetting itself after a profound trauma.
Navigating the Sylvian Fissure
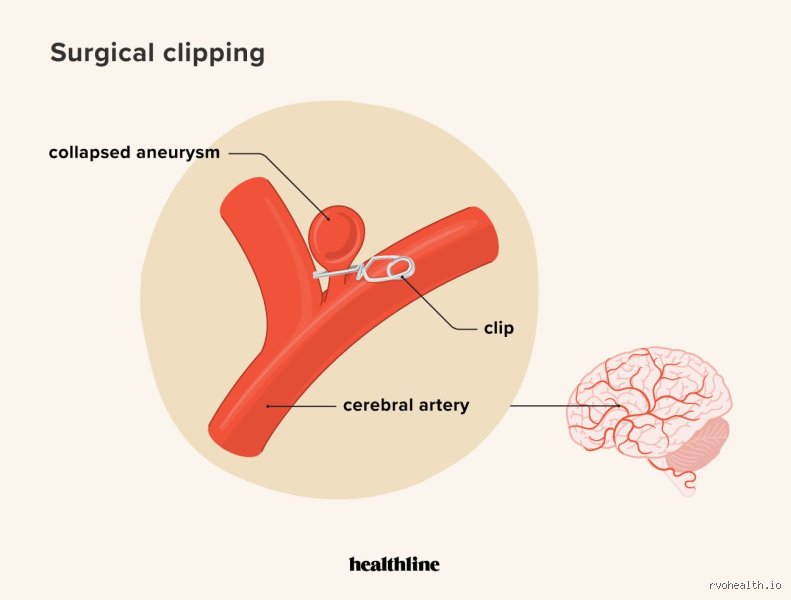
To get to the middle cerebral artery or the internal carotid—the usual suspects for aneurysms—surgeons often have to "split" the Sylvian fissure. This is a natural fold in the brain, but retracting the delicate lobes to gain access can cause "retraction injury." This is where it gets tricky. Even if the surgeon is perfect, the mere act of holding brain tissue aside for three to six hours can disrupt microcirculation. As a result: patients might wake up with temporary hemiparesis (weakness on one side) or aphasia, where words feel like they are stuck behind a thick glass wall. These aren't necessarily permanent "damage," but they are terrifying hurdles that define the first 72 hours of post-operative life.
Neurological Turbulence: Common Immediate Post-Operative Side Effects
The Threat of Cerebral Vasospasm
The most dangerous side effect of aneurysm clipping doesn't actually happen during the surgery itself, but in the days following it. Cerebral vasospasm—a sudden narrowing of the brain's arteries—occurs in roughly 30% to 70% of patients who have suffered a prior rupture, though it can still haunt those who had "cold" elective clippings. Think of the artery as a garden hose that suddenly kinks itself shut because it was irritated by the presence of blood or surgical manipulation. If the brain doesn't get enough blood, a delayed ischemic stroke can occur. This is why you’ll see patients in the ICU being monitored with Transcranial Doppler (TCD) ultrasounds every single morning. It’s a high-stakes waiting game that usually peaks between day 4 and day 14. That changes everything about the recovery timeline, turning a five-day hospital stay into a three-week marathon of hydration and calcium channel blockers like Nimodipine.
Seizures and Cortical Irritability
And then there is the electricity. The brain is an electrochemical machine, and surgery is a massive short-circuiting event. Because the incision and the clip itself can irritate the cerebral cortex, the risk of post-operative seizures is a constant shadow. Statistics suggest that about 5% to 10% of neurosurgical patients might experience at least one seizure in the aftermath. Most hospitals will preemptively put you on Levetiracetam (Keppra), which comes with its own delightful side effects like "Keppra-rage" or profound irritability. It’s a frustrating trade-off. Do you risk a seizure that could blow the surgical site, or do you deal with the mood swings that make you want to throw your hospital tray across the room? Honestly, it's unclear which is worse for the patient's immediate mental health, but the clinical choice is always safety first.
Vision Disturbances and Cranial Nerve Palsy
If the aneurysm was located near the posterior communicating artery, the clip might sit uncomfortably close to the third cranial nerve. This leads to a specific, and frankly annoying, side effect: ptosis (a drooping eyelid) or diplopia (double vision). You might find yourself looking at a world that is permanently out of focus or split in two. Is it permanent? Usually no, as the nerve typically recovers once the initial surgical swelling subsides, but living with an eye patch for three months is hardly the "back to normal" most patients envision. But we're far from a simple fix here, as nerve regeneration moves at the glacial pace of about one millimeter per day.
The Cognitive Toll: Why "Successful" Surgery Doesn't Always Feel Successful
The Fog of Executive Dysfunction
Ask any survivor about the side effects of aneurysm clipping, and they won't talk about the titanium; they’ll talk about the "fog." This isn't just being tired. It is a profound, soul-crushing exhaustion where deciding what to eat for lunch feels like solving a multivariable calculus equation. We call this executive dysfunction. The brain’s frontal lobes, often affected by the surgical approach, struggle to organize, prioritize, and initiate tasks. You might find yourself standing in the middle of the kitchen, forgetting why you opened the fridge. This issue remains one of the most under-reported complications because it doesn't show up on a standard MRI scan. The anatomy looks perfect, but the "software" is glitchy. Why does this happen? It’s likely a combination of the general anesthesia—which, for a ten-hour surgery, is a massive metabolic hit—and the disruption of the delicate white matter tracts that connect different regions of the brain.
Emotional Lability and Personality Shifts
Except that the physical recovery is often faster than the emotional one. Many patients report a strange sense of detachment or, conversely, a heightened sensitivity to noise and light. It’s not uncommon for family members to notice that their loved one is "different"—perhaps more impulsive or less patient than before the clipping. This isn't necessarily a "side effect" of the clip itself, but rather a reaction to the neurological insult of the procedure. We tend to view personality as this fixed, ethereal thing, but it’s deeply rooted in the physical health of our neurons. When those neurons are pushed aside or subjected to temporary ischemia, the person that emerges on the other side might have a slightly different edge to them. In short, the surgery saves the life, but the person living that life might need time to re-introduce themselves to their own brain.
Clipping vs. Coiling: Does the Method Change the Side Effects?
The Invasive Nature of the Clip
When comparing side effects of aneurysm clipping to endovascular coiling, the difference usually comes down to the "insult" to the skull and brain surface. Clipping is invasive. There’s no getting around it. You have a scar, you have missing bone (briefly), and you have the risk of cerebrospinal fluid (CSF) leaks. If the dura doesn't seal perfectly, fluid can leak out, leading to "low-pressure headaches" that only get better when you lie flat. This is a complication unique to the open-surgical approach. Coiling, which goes through the groin, avoids this entirely, yet it carries its own set of risks, like thromboembolic events or the need for long-term blood thinners. Which explains why some patients prefer the "one and done" nature of the clip, despite the more brutal initial recovery.
Long-Term Stability and the Peace of Mind Factor
The thing is, the "side effects" of coiling often include the anxiety of "recurrence," as coils can pack down over time, requiring a second procedure in about 20% of cases. Clipping, however, is almost always a permanent fix. Does the physical trauma of the surgery outweigh the psychological benefit of knowing the aneurysm is definitely "dead"? Experts disagree. Some argue that the lower morbidity of coiling makes it the gold standard, while others point out that for a 40-year-old patient, the long-term durability of a clip is worth the six months of post-operative headaches. As a result: the choice of procedure often dictates the flavor of the side effects you’ll be dealing with for the next year of your life. It’s a trade-off between the body's integrity and the mind's peace.
Common mistakes and misconceptions
The myth of the instantaneous recovery
You might imagine that once the titanium bridge pins that vessel shut, the ordeal evaporates. It does not. Many patients conflate the mechanical success of the intracranial aneurysm ligation with immediate functional restoration, yet the brain remains a temperamental organ that resents being handled. The problem is that the retraction of neural tissue during surgery often induces a localized "stun" effect. This leads to a profound, bone-deep fatigue that can linger for months, which explains why surgeons often see patients weeping in follow-up appointments not from pain, but from sheer exhaustion. We are talking about a metabolic crisis at the cellular level where the brain is literally relearning how to manage its energy reserves. Let's be clear: a successful clip does not mean a quiet Tuesday next week.
Confusing focal deficits with permanent damage
Is the presence of a drooping eyelid or a slight slurring of speech after the procedure a sign of failure? Not necessarily. Post-operative edema—swelling—is a frequent culprit that mimics the symptoms of a stroke without the permanent death of neurons. Because the skull is a rigid vault, even a 3-millimeter shift in tissue due to fluid accumulation can temporarily disrupt signal transmission. As a result: patients often panic, assuming their cognitive or motor trajectory is fixed. Data suggests that up to 15% of patients experience these transient neurological "hiccups" that resolve as inflammation recedes over a six-week window. The issue remains that the internet often catalogs these side effects of aneurysm clipping as permanent disabilities, which creates an atmosphere of unnecessary terror for the convalescing individual.
The silent catalyst: Neuro-inflammation and the "Chemical Storm"
The invisible side effects of aneurysm clipping
Beyond the physical metal of the clip, there is a chemical ghost in the machine. When a surgeon enters the subarachnoid space, the mere presence of microscopic blood droplets or even the irrigation fluid can trigger a sterile inflammatory response. This is the little-known aspect of recovery that dictates your mood and personality changes. But why does a vascular repair make you snap at your spouse? This neuro-inflammation affects the limbic system, the brain's emotional switchboard. Except that most clinical literature focuses on the plumbing—the blood flow—rather than the electrical and chemical atmosphere of the brain. Statistics from postoperative surveys indicate that nearly 40% of survivors report increased irritability or "brain fog" that doesn't show up on a standard CT scan. We must stop treating the brain