Understanding the False Aneurysm: Why Geometry Matters More Than Chemistry
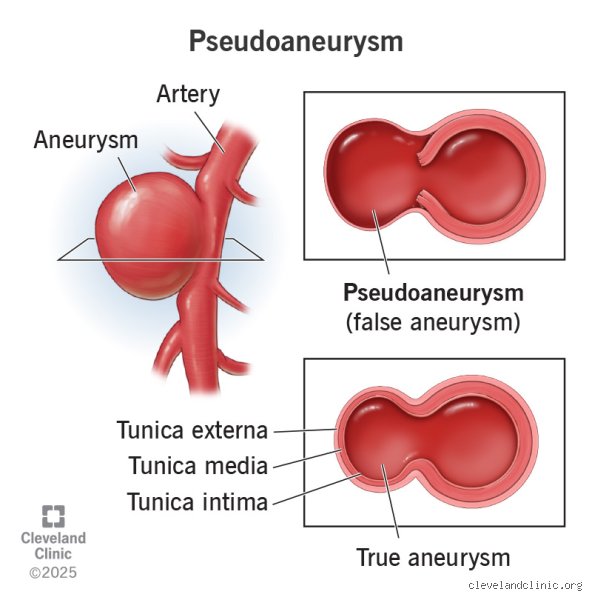
A pseudoaneurysm, or "false aneurysm," is a bit of a medical misnomer that confuses patients and junior residents alike. Unlike a true aneurysm, which involves a weakened but intact bulging of all three layers of the arterial wall, a pseudoaneurysm is essentially a pulsatile hematoma contained only by the surrounding soft tissue or a thin layer of adventitia. Imagine a garden hose with a needle prick that sprays water into a balloon of mud—that is your artery leaking into a localized pocket of tissue. Because the structural integrity of the vessel is compromised, the issue remains one of fluid dynamics and pressure gradients rather than simple inflammation or biochemical imbalance. Most of these occur after femoral artery catheterization, a common reality in modern cardiology where a 6-French sheath might leave a stubborn exit wound.
The Anatomy of a Leak
The blood enters this "false" sac during systole and often exits back into the artery during diastole, creating a swirling, turbulent mess that radiologists call the "yin-yang sign" on Doppler ultrasound. You might find it interesting that the neck of the pseudoaneurysm—the narrow channel connecting the artery to the sac—is the most important feature for any doctor. If that neck is long and narrow, the chance of spontaneous healing goes up, but if it is short and wide, we are looking at a much more volatile situation. I’ve seen cases where a tiny 1-centimeter leak becomes a 5-centimeter crisis in a matter of hours because the patient’s blood pressure was poorly controlled. It is a terrifying race against the tensile strength of human flesh.
Incidence Rates and the Iatrogenic Reality
Data from the Journal of Vascular Surgery suggests that post-catheterization pseudoaneurysms occur in roughly 0.2% to 8% of procedures, depending on the complexity of the intervention and the size of the equipment used. While it sounds rare, consider that millions of these procedures happen annually in the United States alone. The issue isn't just the hole; it is the fact that many of these patients are already on anticoagulants like Heparin or Warfarin, which turns a minor leak into a persistent fountain. When the body's natural "glue" is chemically disabled by therapy, the pseudoaneurysm finds a foothold and refuses to quit. It is a paradox where the treatment for the heart often creates the disaster in the leg.
The Pharmaceutical Heavy Hitter: Bovine Thrombin and the Art of Clotting
If we have to name the "medication" that truly defines pseudoaneurysm treatment, it is Thrombin (Thrombin-JMI). This isn't a drug you pick up at a pharmacy; it is a powerful enzyme that converts fibrinogen to fibrin, effectively creating an instantaneous internal scab. Back in the 1990s, doctors used to spend hours manually compressing a patient’s groin—a brutal, painful process for everyone involved—until Liau and colleagues popularized ultrasound-guided thrombin injection (UGTI) around 1997. This changed everything because it allowed for a precision strike. We inject the enzyme directly into the sac under real-time visualization, watching the blood turn to a solid plug in seconds. It feels like magic, yet it carries the terrifying risk of distal embolization if even a drop of that thrombin leaks back into the main artery.
Navigating the Dangers of Thrombin Injection
But where it gets tricky is the dosage and the source of the enzyme. Most facilities use bovine-derived thrombin, which can rarely trigger anaphylactic reactions or the development of antibodies that cross-react with human Factor V. Because of this, some centers have migrated toward human-recombinant thrombin to avoid the "mad cow" era anxieties, though the cost-benefit analysis is still a point of heated debate in hospital boardrooms. The standard dose usually ranges from 100 to 1,000 units per milliliter, and the goal is to hit the center of the sac while staying far away from the neck. If the thrombin enters the femoral artery, you aren't just treating a leak anymore; you are causing a massive stroke or a limb-threatening clot that requires immediate surgery. Honestly, it’s unclear why we don't use more synthetic sealants, but thrombin's track record is hard to argue with.
Pre-Procedure Sedation and Local Anesthetics
Before the needle ever touches the skin for a thrombin injection, the patient needs a pharmacological buffer. We aren't just being nice; Lidocaine 1% or 2% is vital to numb the tract because the pressure of the injection can be intensely uncomfortable. Some patients, especially those already traumatized by the initial cardiac procedure, require intravenous Midazolam (Versed) or Fentanyl to manage the anxiety and the vasovagal response that often accompanies vascular manipulation. But we have to be careful—oversedating a patient with a potential vascular rupture is a recipe for a respiratory disaster. It’s a delicate dance of keeping them still enough for the ultrasound tech to get a clear image while ensuring they are awake enough to tell us if their foot suddenly goes numb.
Supporting Medications: Managing the Systemic Environment
While thrombin does the heavy lifting, the "medication used for pseudoaneurysm" list must include antihypertensives. If a patient’s systolic blood pressure is screaming at 180 mmHg, no amount of thrombin or manual pressure will keep that hole closed. We often reach for short-acting beta-blockers like Esmolol or Nitroglycerin drips to bring the pressure down to a manageable 120 mmHg. This reduces the "wall stress" on the injured artery. Think of it like trying to patch a tire while the car is still driving at 80 miles per hour; you have to slow down before the patch has any hope of sticking. People don't think about this enough, but blood pressure management is arguably more "essential" than the thrombin itself in the long-term recovery phase.
Antibiotics and the Risk of Mycotic Pseudoaneurysms
When a pseudoaneurysm is caused by infection—often seen in IV drug users or after a contaminated surgical site—it is called a mycotic pseudoaneurysm. Here, the pharmacological strategy shifts violently from clotting to killing bacteria. Vancomycin and Ceftriaxone are the standard heavy hitters used to stabilize the vessel wall by reducing the enzymatic destruction caused by pathogens like Staphylococcus aureus. In these cases, injecting thrombin is often a bad idea because you’re just creating a localized "nest" for the bacteria to grow in. You cannot fix a structural leak in a rotting pipe with just glue; you need to treat the rot first. As a result: the medication becomes the primary therapy, often for 6 weeks or more, while we wait for the tissue to become healthy enough for a surgical graft.
The Role of Antiplatelet Adjustment
We're far from it being a simple "add a drug" situation; sometimes the best medication management is stopping a drug. If a patient is on a P2Y12 inhibitor like Clopidogrel (Plavix) or a GP IIb/IIIa inhibitor like Abciximab, the pseudoaneurysm is significantly less likely to close on its own. Doctors have to weigh the risk of a stent in the heart clotting off against the risk of the leg bleeding out. It is a brutal clinical tightrope. In some cases, we might administer Protamine Sulfate to reverse the effects of Heparin, but this is a "sharp opinion" move that can lead to catastrophic thrombosis elsewhere. We are constantly trading one risk for another, hoping the patient's biology is forgiving enough to handle the compromise.
Medication vs. Mechanical Compression: The Great Debate
For decades, Ultrasound-Guided Compression (UGCR) was the gold standard, but it was a miserable experience. It involved a clinician pressing an ultrasound probe against a patient’s groin for 20-minute intervals, often for over an hour, trying to physically collapse the neck of the sac. Compared to this, thrombin injection is a dream. Yet, some conservative old-school surgeons still argue for compression in small leaks (under 2 cm) because it avoids the $1,500 price tag of a thrombin kit and the risk of an embolic event. I disagree with the "compression first" dogmatic approach for everything. Why put a patient through an hour of agony when a 30-second injection has a 96% success rate? The issue remains that we prioritize "non-invasive" labels over the actual patient experience, which explains why UGTI has largely won the popularity contest in modern vascular labs.
When Oral Medications Fail: The Threshold for Surgery
There is a point where we have to admit the limits of chemistry. If the pseudoaneurysm is larger than 4 or 5 centimeters, or if the skin is starting to thin and turn dusky (a sign of impending rupture), we stop reaching for the needle and start calling the OR. Medications can't fix a compartment syndrome where the leaked blood is crushing the nerves in the leg. In these high-stakes moments, the only medication that matters is the General Anesthesia used to put the patient under so a surgeon can physically sew the artery shut. We have to be honest: while thrombin is an incredible tool, it is a localized fix for a localized problem, and it fails spectacularly when the arterial defect is too jagged or the patient's coagulation system is too far gone. It’s a tool, not a panacea, and recognizing that distinction is what keeps patients alive.
Common Myths and Clinical Blunders
The Dangerous Allure of Watchful Waiting
You might think a small leak will just plug itself if we give it enough time, like a minor plumbing drip in a basement. The problem is that a femoral artery pseudoaneurysm lacks a true vessel wall, meaning it is nothing more than a pressurized hematoma masquerading as a stable structure. We often see practitioners assuming that every small sac under 2 centimeters will spontaneously thrombose without intervention. While some do, ignoring a pulsating mass because it looks "unimpressive" on a duplex scan is a recipe for disaster. Let's be clear: waiting is not a passive act but a calculated risk that can lead to skin necrosis or catastrophic rupture. If the neck of the lesion is wide, no amount of patience will magically seal that gap. And would you really gamble a patient's limb on a coin flip?
Misunderstanding the Role of Oral Anticoagulants
There is a persistent misconception that simply stopping a patient's aspirin or warfarin will instantly resolve the iatrogenic vascular injury. Which explains why some clinics delay definitive treatment for days while waiting for an INR to drop. But the structural defect in the arterial wall remains regardless of how thin the blood is. Anticoagulation definitely makes the pulsatile hematoma more likely to expand, yet it does not create the hole; the needle or sheath did that. Resuming these medications too early after a thrombin injection is the most frequent cause of recurrence we see in modern practice. Because the clot formed by bovine thrombin is susceptible to the same fibrinolytic processes as any other plug, timing is everything.
The Forgotten Variable: Thrombin Dose Titration
Precision over Volume
Most clinicians grab a vial of thrombin and assume the goal is to empty the syringe into the sac until the "swish-swish" sound on the Doppler stops. This is primitive. The issue remains that iatrogenic pseudoaneurysm morphology varies wildly between patients. An expert knows that injecting 500 units per mL too rapidly can cause "jetting," where the medication is pushed through the neck and into the systemic circulation. This results in distal embolization, which is a fancy way of saying you just gave your patient a cold, blue foot. We advocate for a "staccato" injection technique. You inject a tiny aliquot, wait ten seconds, and observe the layering of the thrombus. It is an art form, not just a procedure. (Honestly, some surgeons still treat it like they are filling a pothole with cement). Success requires visualizing the neck of the pseudoaneurysm and ensuring the needle tip is as far from the native artery as possible to prevent inadvertent thrombosis of the main channel.
Frequently Asked Questions
What is the success rate of ultrasound-guided thrombin injection?
Modern clinical data suggests that ultrasound-guided thrombin injection boasts a primary success rate between 91% and 98% for simple lesions. In a retrospective study of 240 patients, only 5% required a second injection to achieve complete occlusion of the vascular false aneurysm. As a result: this has become the gold standard over the older, more painful method of manual compression which often took 30 to 60 minutes of intense pressure. We see failures most often in patients with extremely large sacs exceeding 5 centimeters or those on aggressive dual-antiplatelet therapy. In short, if the first attempt fails, a second pass usually does the trick before surgery is even mentioned.
Can medication alone ever replace a physical procedure?
No pill or intravenous drip exists that can travel through the bloodstream and specifically target the site of arterial perforation. While we use bovine thrombin or human-derived clotting factors, these are topically applied agents injected directly into the pathology, not systemic drugs. Except that some might argue aggressive blood pressure control is a form of medical management, it only prevents the sac from growing rather than fixing the hole. You cannot medicate a mechanical failure of a blood vessel wall. Therefore, "medication" in this context always refers to the clotting agents used during an interventional procedure.
What are the signs that a pseudoaneurysm is worsening despite treatment?
Patients must watch for a rapid increase in localized swelling or a change in the color of the skin over the groin puncture site. If the area becomes tight, shiny, or intensely painful, it suggests the pseudoaneurysm sac is expanding and putting pressure on the overlying tissue or nearby nerves. You should also check for "pins and needles" sensations in the foot, as this indicates the hematoma is compressing the femoral nerve. A decrease in the temperature of the leg is an absolute emergency. These symptoms mean the localized problem is becoming a systemic threat to the limb's viability.
A Final Word on Vascular Vigilance
The medical community must stop viewing the pseudoaneurysm as a nuisance and start seeing it as a sentinel event of technical failure. We rely too heavily on the "safety net" of thrombin while ignoring the precision required during the initial arterial access. It is my firm stance that every cardiac cath lab should have a dedicated post-procedure protocol that moves beyond simple palpation. Relying on "feeling a pulse" is antiquated when portable duplex technology is readily available. We have the tools to eliminate these complications almost entirely. If we continue to treat vascular complications as inevitable, we fail our patients. The focus must shift from how we fix the leak to how we prevent the puncture from failing in the first place.