Understanding the Anatomy of a Breakdown: What Is Pancreatitis Exactly?
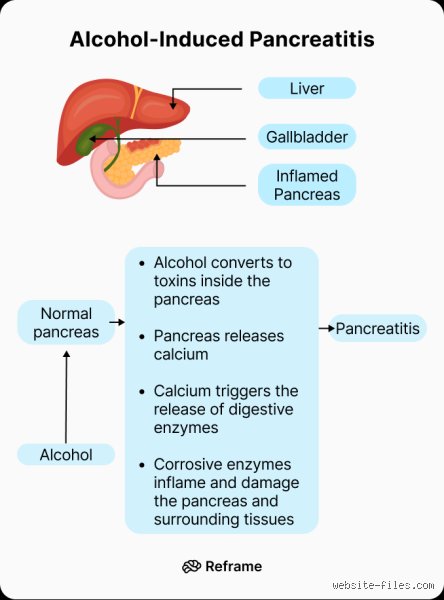
To get why booze wreaks such havoc, you have to look at the pancreas as a high-stakes chemical factory. It sits tucked behind the stomach, quietly pumping out digestive enzymes like lipase and protease that stay inactive until they hit the small intestine. Except that alcohol disrupts this safety protocol. When the system fails, these enzymes activate while they are still inside the organ, effectively causing the pancreas to eat itself. It sounds like something out of a horror movie, right? But the thing is, this "autodigestion" is the fundamental mechanism behind the agonizing pain that sends over 275,000 Americans to the hospital every year for acute episodes.
The Invisible Scarring of Chronic Inflammation
While an acute attack feels like a sudden lightning strike in your abdomen, the chronic version is a slow, agonizing burn. It is a persistent inflammatory state that turns soft, functional tissue into hard, useless fibrotic scars. I’ve seen patients who think they’ve "recovered" from a binge, only to have stellate cells in their pancreas permanently flipped into a collagen-producing overdrive. This isn't just a temporary swelling. It is the architectural restructuring of an organ that eventually loses its ability to produce insulin, leading to what we call Type 3c diabetes. People don't think about this enough—the fact that your happy hour habit could literally rewire your endocrine system until it breaks.
The Threshold Myth and Individual Sensitivity
How much is too much? Doctors used to cite a "threshold" of five drinks a day for five years, but we're far from such a simple math equation now. Recent longitudinal studies suggest that for some, even moderate social drinking acts as a "second hit" to an underlying genetic predisposition. Because our bodies process toxins at different speeds, a "safe" amount for one person might be a cytotoxic death sentence for another's acinar cells. Yet, the medical community still clings to these generalized averages, which explains why so many early-stage cases go undiagnosed until the damage is visible on a CT scan.
The Molecular Mayhem: How Ethanol Turns Into a Biological Weapon
Alcohol doesn't just "irritate" the pancreas; it launches a multi-pronged molecular assault. When you take a sip, your body works frantically to break down ethanol, primarily using two pathways: oxidative and non-oxidative. The oxidative route creates acetaldehyde, a nasty, reactive chemical that generates free radicals like a broken sparkler. These free radicals go on a rampage, stripping electrons from cell membranes and causing what scientists call oxidative stress. The issue remains that the pancreas has a very limited supply of antioxidants compared to the liver, making it uniquely vulnerable to this chemical shrapnel.
The Non-Oxidative Trap and Fatty Acid Ethyl Esters
Where it gets tricky is the non-oxidative pathway, which produces fatty acid ethyl esters (FAEEs). These compounds are particularly toxic to the mitochondria—the powerhouses of your cells. When FAEEs accumulate, they cause a massive leak of calcium within the pancreatic acinar cells. This calcium surge is the "master switch" that prematurely turns on those dormant digestive enzymes I mentioned earlier. And once that switch is flipped, the cascade is almost impossible to stop without medical intervention. As a result: the cell's internal machinery collapses, leading to necrosis, which is just a clinical way of saying the tissue is dying in real-time.
Blood Flow and the Ischemic Squeeze
Beyond the chemistry, there is the plumbing. Alcohol causes the tiny blood vessels in the pancreas to constrict while simultaneously increasing the viscosity of pancreatic secretions. Imagine trying to push thick sludge through a narrowing pipe—it's a recipe for a backup. This localized hypoxia (lack of oxygen) further weakens the cells, making them even less capable of resisting the toxic effects of the booze. But why does this happen to the guy at the end of the bar and not his friend? Honestly, it’s unclear, though researchers are currently looking at the SPINK1 and CFTR gene mutations as the likely culprits for this uneven distribution of misery.
Diagnostic Deceptions: Why Alcohol-Induced Pancreatitis is Often Missed
Medical students are taught to look for "boring" symptoms: epigastric pain radiating to the back, nausea, and vomiting. Except that alcohol-induced cases often present with a much more "smoldering" profile that can mimic simple acid reflux or a gallbladder issue. Patients often downplay their intake—which is a whole different sociological problem—but even honest reporting doesn't always help. In the early stages of alcoholic chronic pancreatitis, your lipase levels might not even be significantly elevated because the organ is too scarred to produce them anymore. That changes everything for a doctor relying solely on blood work.
The False Security of Clear Imaging
You might go to the ER, get an ultrasound, and be told everything looks "fine." Don't bet your life on it. Transabdominal ultrasounds are notoriously bad at seeing through the gas and fat that often surround the pancreas. By the time a standard MRI shows parenchymal atrophy or calcification, you have likely lost over 60% of your organ's function. In short, a "clean" scan in a regular drinker is often just a sign that the technology isn't sensitive enough to catch the microscopic fire raging under the surface. We need to stop treating a lack of visible evidence as a clean bill of health.
Alcohol vs. Gallstones: A Comparison of Two Different Evils
It is worth noting that gallstones remain the number one cause of acute attacks, usually by physically blocking the common bile duct. But the pathology between the two is night and day. Gallstone pancreatitis is an obstructive mechanical failure; you remove the stone, and the pancreas usually recovers quite well. Alcohol is different. It is a metabolic poison that alters the very biology of the cells. While a stone is a one-time accident, alcohol is a recurring systemic threat that lingers in the tissues long after the last drink has been processed.
Recovery Trajectories and Recurrence Rates
The data from the 2023 National Clinical Database shows a startling trend: patients with gallstone-induced attacks have a recurrence rate of less than 10% if they have their gallbladder removed. Contrast that with alcohol-related cases, where the recurrence rate jumps to nearly 50% within two years if the patient continues to drink. This isn't just about "willpower"—it's because the alcohol has already primed the inflammatory pathways. Once that inflammatory "memory" is established, even a small amount of booze can trigger a massive, disproportionate response. The biological stakes are simply higher when ethanol is the driver.
Common Myths and Clinical Misconceptions
The Illusion of the Safe Minimum
We often comfort ourselves with the fairy tale that only the stereotypical, street-dwelling alcoholic faces a rotting pancreas. The problem is that biology ignores social status. Many patients assume a nightly bottle of wine is benign because it fits a refined lifestyle. Yet, acinar cell sensitization occurs at much lower thresholds than the public realizes. If you believe your craft beer habit is shielded by its high price tag, you are mistaken. Data from longitudinal studies indicate that consuming as little as 40 grams of ethanol daily—roughly three standard drinks—can significantly elevate the risk of chronic architectural changes. The organ does not care about the vintage; it cares about the cumulative metabolic tax. Because the pancreas possesses a limited capacity to regenerate, every inflammatory episode acts like a permanent scar on a finite canvas.
The "Clear Liquid" Fallacy
There is a persistent, dangerous rumor that clear spirits like vodka are "cleaner" and less likely to trigger flares. Let's be clear: the ethanol molecule is the primary culprit, regardless of whether it arrives draped in juniper berries or potato starch. While congeners in darker spirits might worsen a hangover, the metabolic pathway of non-oxidative metabolism remains identical. People frequently ask if switching to white wine will save them. It won't. In fact, some researchers suggest that the high sugar content in mixers or specific ferments might exacerbate hypertriglyceridemia, a known co-factor in organ failure. And this brings us to the reality that a "clean" drink is an oxymoron when discussing glandular toxicity. Can alcohol cause pancreatitis even if it is top-shelf? Absolutely, and often with more speed than the casual drinker anticipates.
The Genetic Roulette: An Expert Perspective
The PRSS1 and SPINK1 Variables
Why does one person drink for decades with nothing but a fatty liver, while another develops a necrotic nightmare after three years of heavy partying? The answer lies in the silent architecture of your DNA. The issue remains that we are not all born with the same defensive hardware. Mutations in the PRSS1 gene or variants in the SPINK1 inhibitor act like a hairline fracture in a dam. When you introduce ethanol into a system with these predispositions, you aren't just drinking; you are lighting a fuse on a pre-existing bomb. As a result: the threshold for trypsin activation drops precipitously. Most people have no idea they carry these variants until the first agonizing ambulance ride. (It is a terrifying way to learn about your ancestry.) If we could screen every teenager, we might see a drastic shift in lifestyle choices, but the current medical landscape isn't there yet. We must acknowledge the limit of our foresight; we cannot predict with 100% certainty who will break first.
Frequently Asked Questions
Does a single binge-watching session with heavy drinking cause permanent damage?
A solitary episode of extreme intoxication, often defined as five or more drinks in a sitting, can indeed trigger acute edematous pancreatitis. While a single event might resolve without visible scarring, clinical imaging often reveals microscopic parenchymal changes that persist long after the pain fades. Statistics show that roughly 10% to 15% of acute cases transition into a chronic state if the behavior is repeated. The initial flare is frequently a warning shot from a system that is struggling to neutralize reactive oxygen species. Consequently, the danger is not just the immediate pain but the silent "priming" of the organ for future collapse.
Is it possible to reverse the damage by quitting entirely?
The human body is resilient, but the pancreas is notoriously unforgiving compared to the liver. If the damage is caught in the early acute phase, complete cessation of drinking can prevent the progression to fibrotic tissue replacement. However, once the organ reaches the stage of calcific chronic pancreatitis, the structural changes are largely irreversible. You can stop the fire from spreading, but you cannot un-burn the wood that has already turned to ash. Data suggests that patients who quit immediately after their first attack have an 80% lower recurrence rate than those who attempt "moderate" consumption later. In short, sobriety is the only proven method to halt the necrotic slide.
How long after drinking does the pain usually start?
The timeline is often shorter than most expect, typically manifesting between 6 to 24 hours after the final glass. This delay occurs because the inflammatory cascade requires time for enzyme premature activation to reach a critical mass. You might fall asleep feeling fine, only to wake up at 4:00 AM with a sensation often described as a hot iron being pushed through the abdomen. Can alcohol cause pancreatitis symptoms to appear days later? It is less common, as the oxidative stress usually peaks shortly after the blood alcohol concentration begins to drop. Most emergency room admissions for this condition spike during the early morning hours following weekend festivities.
The Verdict: Biology Over Bravado
We need to stop treating the pancreas like a secondary character in the drama of addiction. It is the protagonist of your metabolic survival, and it is remarkably fragile. The medical community often tip-toes around the hard truth, but I will not: there is no such thing as a "safe" amount of liquor for a sensitized system. Which explains why the only logical stance is one of radical prevention. If you have felt that dull ache beneath your ribs, the window for negotiation is closing fast. We must prioritize organ integrity over social lubrication every single time. The irony is that we spend thousands on organic food and gym memberships while pouring a known solvent over our most delicate internal machinery. Stop looking for a loophole that doesn't exist.