Beyond the Breath: Why Defining the Four Stages of COPD is a Moving Target
When we talk about lung health, we often treat it like a fuel gauge where the needle only moves in one direction. But the thing is, the way we categorize these stages relies heavily on a metric called spirometry. This test measures how much air you can huff out, yet it fails to capture the sheer exhaustion of a "good" day versus a "bad" day. Experts disagree on whether these numerical buckets actually help patients, or if they just make insurance billing easier for the clinics. Some clinicians argue that focusing too much on the FEV1/FVC ratio—which must be below 0.70 to even get a diagnosis—ignores the person sitting in the chair who can’t walk to their mailbox despite having "mild" numbers. I believe we rely far too much on the machines and not enough on the patient's lived experience of breathlessness.
The Shadow Pandemic of Undiagnosed Lung Damage
There is a massive gap in how we identify early disease. Statistics from the American Lung Association suggest that upwards of 12.5 million Americans are diagnosed, but millions more are walking around with Stage 1 Mild COPD without a clue. Why? Because the human body is incredibly good at compensating for failure until it isn't. You might stop taking the stairs or blame a "smoker's cough" on the weather, effectively self-adjusting your life to hide the damage from your own consciousness. By the time someone actually sits in a specialist's office in 2026, they’ve often lost 50% of their lung capacity already. It is a bit like realizing your house is on fire only after the roof collapses—hardly an ideal time to start looking for a garden hose.
The GOLD Standard: Decoding the Technical Framework of Airflow Limitation
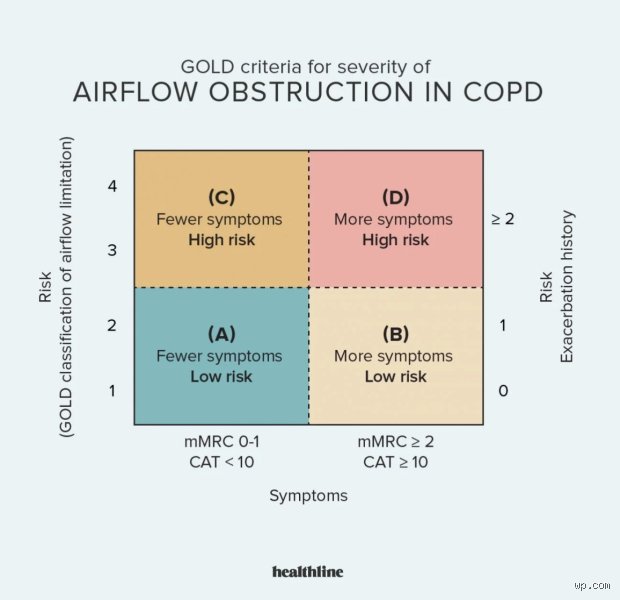
To understand the progression, we have to look at the GOLD staging system, which was updated significantly to move away from just looking at airflow to looking at symptoms and exacerbations. The technical progression is categorized by the percentage of predicted FEV1. In Stage 1, your FEV1 is 80% or higher. By the time you hit Stage 2, it’s between 50% and 79%. Stage 3 sees a drop to 30-49%, and Stage 4 is anything less than 30%. But here is where it gets tricky: two people can have the exact same 45% FEV1 (Stage 3), yet one might be hospitalized every month while the other still plays golf with a portable oxygen concentrator. This discrepancy led to the creation of the ABCD assessment tool, which layers symptom severity on top of the raw numbers.
The Physics of Obstructed Airways
What is actually happening inside the bronchioles and alveoli during these transitions? In a healthy lung, the air sacs are like tiny, stretchy balloons. In COPD, particularly in emphysema, those balloons lose their elasticity and eventually pop, creating large, useless air pockets called bullae. This leads to air trapping. You can’t get the old air out, so there is no room for the fresh, oxygen-rich air to come in. Imagine trying to breathe while someone is hugging your chest as hard as they can. That changes everything. The diaphragm, which should be a dome-shaped muscle doing the heavy lifting, gets flattened out by the over-inflated lungs and loses its mechanical advantage. It’s a structural disaster that starts as a microscopic inconvenience.
Quantitative Data and the 2026 Clinical Reality
Looking at the data, the BODE Index is often a better predictor of mortality than the GOLD stages alone. This index looks at Body Mass Index, Airflow Obstruction, Dyspnea (breathlessness), and Exercise Capacity. Why does this matter? Because a patient in Stage 2 with a low BMI and high breathlessness might actually be at higher risk than a Stage 3 patient who exercises daily. In 2024, a landmark study published in the Lancet pointed out that lung function decline is not linear. Some people are "rapid decliners" who lose 100mL of lung capacity per year, while others stay stable for a decade. Honestly, it's unclear why some lungs give up the ghost so much faster than others, though genetics and alpha-1 antitrypsin deficiency certainly play their parts in the background.
Stage 1 and 2: The Subtle Creep of Mild and Moderate Obstruction
In the beginning, COPD is a ghost. Stage 1 is often characterized by nothing more than a persistent cough that produces sputum. You might feel a bit winded during a brisk walk, but you tell yourself you're just getting older or need to hit the gym more often. The GOLD 1 classification is essentially a warning shot that almost everyone ignores. But then Stage 2 hits, and that’s where the "moderate" label feels like a bit of an understatement. This is typically when people finally seek medical help because the shortness of breath starts interfering with daily chores like grocery shopping or vacuuming. At this point, bronchodilators become a staple of the medicine cabinet. We're far from the end of the road here, yet this is the most critical window for intervention to stop the slide into disability.
The Moderate Stage 2 Milestone
Moderate COPD is the "great realization" phase. Patients start noticing that exacerbations—those frightening flare-ups where breathing becomes nearly impossible—happen after a simple cold or a dusty day in the garden. This is the stage where pulmonary rehabilitation can have the most profound impact, yet it remains criminally underutilized in many healthcare systems. But the issue remains: the lungs do not regenerate. Once those alveolar walls are gone, they are gone for good. We can optimize what’s left, sure, but we are essentially managing a controlled descent. It’s a sobering reality that many struggle to accept until the supplemental oxygen tanks show up at the front door.
Comparing COPD Stages to Other Chronic Respiratory Conditions
It is worth noting that the four stages of COPD don't look the same as the progression of asthma or pulmonary fibrosis. While asthma is often reversible—meaning your numbers can go back to normal with a puff of an inhaler—COPD is defined by its irreversibility. This is a key distinction that often gets muddled in general health discussions. In Stage 1 or 2, a patient might feel like they have asthma, but the post-bronchodilator test will show that their airways remain stubbornly narrowed. Pulmonary fibrosis, on the other hand, is a "restrictive" disease where the lungs get scarred and stiff, unlike the "obstructive" nature of COPD where the lungs get floppy and over-inflated. Understanding these differences is vital because using the wrong treatment can sometimes do more harm than good, especially if a clinician misses a comorbidity like congestive heart failure which mimics many of these symptoms.
The Diagnostic Overlap and Confusion
The medical community frequently discusses ACO (Asthma-COPD Overlap). This isn't a separate stage, but a complicating factor that can make a Stage 2 patient feel like they are in Stage 4 during an allergy season. Does the staging system handle these outliers well? Not particularly. The rigid nature of the 1-through-4 system often fails to account for the inflammatory "noise" that smokers or people living in high-pollution areas like Delhi or Los Angeles deal with daily. As a result: the diagnosis can feel like a life sentence, but the stage is just a snapshot in time. We need to look at the total lung capacity (TLC) and residual volume (RV) to get the full picture of how much space that "trapped air" is actually taking up in the chest cavity, which often reveals a much more complex story than a simple FEV1 percentage ever could.
Common pitfalls and the trap of the silent onset
Most patients believe that a chronic cough is simply a consequence of aging or perhaps a stubborn remnant of a previous flu. Let's be clear: lungs do not just wear out without a specific physiological insult. Because the initial decline in lung function is often asymptomatic, many people ignore the subtle signal of breathlessness during a steep climb. It is easy to blame the stairs. But this denial creates a massive diagnostic gap where the disease progresses unhindered. The problem is that by the time you actually seek a physician's counsel, you might have already forfeited 50% of your respiratory capacity. Waiting for a "crisis" to occur is a tactical error in managing COPD stages because the damage to the alveoli is permanent and irreversible. We often see people relying on over-the-counter cough suppressants which only mask the inflammation while the underlying obstruction worsens. The issue remains that the medical community still struggles with underdiagnosis; current data suggests that up to 12 million Americans may have the condition without even knowing it.
The myth of the smokers-only club
There is a persistent, almost cruel irony in the assumption that only lifelong heavy smokers suffer from respiratory failure. While tobacco is the primary culprit, nearly 25% of individuals diagnosed with chronic obstructive pulmonary disease have never smoked a single cigarette in their lives. Genetics, specifically Alpha-1 antitrypsin deficiency, can play a devastating role. Environmental factors like biomass fuel exposure or long-term inhalation of industrial dusts in workplaces like mining or textiles are frequently overlooked by general practitioners. Have you considered that your childhood asthma might have paved the legal road for adult lung obstruction? It is a possibility that complicates the clinical picture. The issue remains that focusing solely on smoking history leads to missed opportunities for early intervention in non-smokers who are suffering from significant airflow limitation.
The misunderstanding of oxygen therapy
Many patients view a portable oxygen tank as a surrender or a final admission of defeat. This is a profound misconception. Using supplemental oxygen is not a sign of impending death; rather, it is a tool for maintaining systemic organ health. Chronic hypoxia—low oxygen levels in the blood—forces the heart to work significantly harder, leading to pulmonary hypertension and eventual right-sided heart failure. In short, the tank protects your heart. Yet, many resist this intervention due to social stigma or the false belief that their lungs will "get lazy" if they use it. Except that lungs are not muscles; they are gas exchange organs that are physically failing, and starving them of oxygen only accelerates the decline.
The hidden impact of skeletal muscle dysfunction
Expert clinicians now look far beyond the chest cavity to understand the full scope of the disease. We must recognize that systemic inflammation doesn't stay confined to the bronchioles. As the disease advances through the GOLD stages, the body enters a catabolic state where it begins to break down muscle tissue for energy. This is why many late-stage patients experience profound weight loss and "muscle wasting." The diaphragm, the primary muscle of respiration, becomes flattened and inefficient due to lung hyperinflation. As a result: your peripheral muscles in the legs and arms also weaken, making even simple tasks feel like a marathon. Which explains why pulmonary rehabilitation focuses so heavily on strength training rather than just "breathing exercises." You cannot fix the lungs, but you can certainly make the "pumps" (your muscles) more efficient. (Note: physical activity remains the single best predictor of survival across all categories). But staying active requires a level of discipline that many find daunting when every breath feels like sucking air through a tiny straw.
The neurobiology of breathlessness
There is an often-ignored psychological feedback loop between the brain and the lungs. When you cannot catch your breath, the amygdala triggers a "fight or flight" response. This sudden surge of adrenaline increases your heart rate and makes you breathe faster, which—ironically—traps even more air in the lungs and worsens the sensation of dyspnea. It is a biological trap. Modern expert advice now includes "pacing" techniques and cognitive behavioral therapy to manage this anxiety. If we can break the panic cycle, we can often reduce the perceived severity of the four stages of COPD without even changing the medication dosage.
Frequently Asked Questions
Can my lung function improve if I stop smoking now?
While the physical scarring of the lung tissue is permanent, the rate of decline in FEV1—the amount of air you can exhale in one second—slows down significantly the moment you quit. Clinical studies show that after 1 year of cessation, the accelerated loss of lung function typical of smokers begins to mirror the natural, slower decline of a healthy non-smoker. Statistics indicate that smoking cessation can add years of life even for those already in Stage 3 or 4. Furthermore, the inflammation in your airways begins to subside within weeks, leading to less mucus production and a reduced frequency of acute exacerbations. It is never a futile effort, regardless of your current age or diagnosis severity.
How do doctors determine which of the four stages of COPD I am in?
Physicians use a diagnostic test called spirometry to measure how much air you can blow out and how fast you can do it. The primary metric is the FEV1/FVC ratio, and if this number is less than 0.70 after taking a bronchodilator, a diagnosis is confirmed. You are classified into Stage 1 if your FEV1 is 80% or more of the predicted value for your age and height. Stage 2 ranges from 50% to 79%, while Stage 3 is between 30% and 49%. If your lung function drops below 30%, you are categorized as Stage 4, which is often called very severe obstruction.
Is a lung transplant a realistic option for most people?
Lung transplantation is a high-risk procedure reserved only for those in the most advanced chronic obstructive pulmonary disease categories who have exhausted all other medical treatments. Data from various registries shows that while the surgery can improve quality of life, the 5-year survival rate for lung transplant recipients is roughly 50% to 60%. Candidates must meet strict criteria, including being otherwise healthy enough to survive the surgery and having a strong support system. Because the supply of donor organs is extremely limited, many patients never make it onto the list. Most experts prefer to focus on bronchoscopic lung volume reduction or specialized valve placements as less invasive alternatives for eligible patients.
A defiant outlook on respiratory management
We need to stop treating this diagnosis as a passive slide toward a ventilator. The current medical paradigm often feels overly focused on the "end" rather than the quality of the journey. Aggressive intervention at Stage 1 or 2 is the only way to rewrite the script of your future. We must be honest: your lungs will never be eighteen again, but that does not mean your life is over. The issue remains that we undervalue the power of holistic lifestyle changes compared to the latest expensive inhaler. I take the firm position that the "severity" of your disease is defined less by a number on a spirometer and more by your willingness to adapt. You are not a set of failing bellows; you are a complex system that can still find efficiency in the face of obstruction. In short, breathe with intent and move with purpose before the choice is taken away.