Beyond the Timer: What We Actually Mean by Sterilization Speed
When people ask about duration, they usually forget that microbial death isn't a light switch you just flip. It is a logarithmic decay. We are talking about a process that must be absolute, because "mostly sterile" is just a fancy way of saying "contaminated." In professional environments, the clock starts long before the machine beeps. I find it fascinating that while we live in an era of instant gratification, the laws of thermodynamics and protein denaturation refuse to be rushed. You can't just "overclock" a vacuum-sealed chamber without risking the integrity of the very tools you are trying to clean. The thing is, the time spent isn't just about killing germs; it is about ensuring the heat or gas actually penetrates the center of a dense linen pack or the narrow lumen of a surgical endoscope. If the middle stays cool, the whole cycle is a failure.
The Myth of the "Quick Wash" and Why Bioburden Matters
How long does sterilization take if the tools are visibly dirty? The answer is: it doesn't matter, because it won't work. Before the timer even begins, technicians must engage in rigorous pre-cleaning. This is where it gets tricky for the uninitiated. If a surgical tray has residual protein or dried blood, those substances act as a physical shield for spores. We're far from a simple "set it and forget it" situation. The initial bioburden count—the number of living organisms on a surface before the process starts—dictates the necessary exposure time. Starting with a million microbes requires a significantly longer "kill time" than starting with a hundred. Because of this, the actual time investment in a sterile processing department (SPD) is often doubled by the manual labor required before the machine even turns on.
Understanding the Log Reduction Factor in Time Calculations
We measure success in "logs." To reach that 10^-6 gold standard, we have to calculate the D-value, which is the time required at a specific temperature to kill 90% of a specific microorganism like Geobacillus stearothermophilus. If the D-value at 121 degrees Celsius is 1.5 minutes, you need at least 18 minutes of exposure to achieve a 12-log reduction. Does that seem overkill? Perhaps, but in a world of antibiotic-resistant "superbugs," that margin of error is the only thing standing between a routine procedure and a life-threatening infection. It is a mathematical certainty applied to a biological nightmare.
The Dominance of Steam: Why Pressure Cooking is Still King
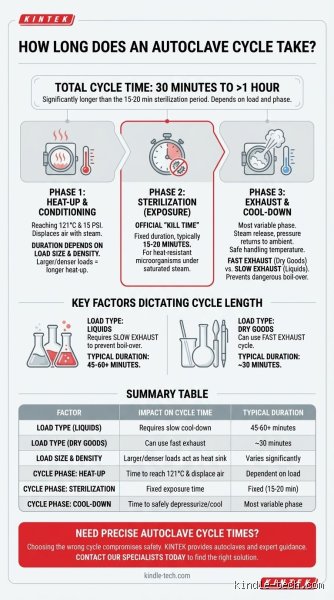
Saturated steam under pressure remains the fastest and most reliable method for most heat-stable items. This is autoclave technology, and it relies on the fact that moist heat is far more efficient at destroying microbial proteins than dry heat. Think about it: you can stick your hand in a 200-degree oven for a second without a burn, but 200-degree steam would scald you instantly. That energy transfer is why steam wins. Most hospitals run their autoclaves at 132 degrees Celsius (270 degrees Fahrenheit). At this temperature, the actual exposure time for wrapped instruments is usually 4 minutes. Yet, the issue remains: the drying phase can take another 20 to 30 minutes. If you pull a pack out while it is still damp, "wicking" occurs, where bacteria from the air or your hands travel through the moisture into the sterile field.
Gravity Displacement vs. Pre-Vacuum Cycles
Not all steam cycles are created equal, and the mechanics change the duration. Gravity displacement cycles are the older, slower cousins. They rely on the fact that steam is lighter than air; as steam enters the chamber, it pushes the air out through a drain at the bottom. This is a slow, passive process that often requires 30 minutes at 121 degrees Celsius. Pre-vacuum sterilizers, however, are the modern workhorses. They use a pump to mechanically suck the air out, creating a vacuum that allows steam to burst into every crevice instantly. This changes everything for complex loads. A pre-vac cycle is faster, more consistent, and much better at handling those annoying "cold spots" that plague gravity units. But even with a vacuum, you can't cheat the physics of heat penetration.
The Critical Role of Temperature Ramping
A common mistake is thinking the cycle starts when you hit "Start." It doesn't. The chamber must reach the validated set point before the exposure timer begins to countdown. Depending on the size of the load—say, a massive 25-pound orthopedic tray—this "come-up time" can take 15 minutes alone. And because we must ensure the coldest part of the load reaches the target temperature, the sensors are placed in the most difficult-to-reach area, usually the drain. But what happens if the steam is too dry? Ironically, "superheated" steam acts like dry air and is less effective, potentially extending the time needed or, worse, failing to sterilize at all. It is a delicate balance of moisture and pressure.
Chemical Sterilization: When Heat is the Enemy
What do you do with a multi-million dollar robotic camera or a plastic catheter that would melt into a puddle in an autoclave? You turn to chemicals, and here, time is no longer your friend. Ethylene Oxide (EtO) is the traditional heavy hitter for heat-sensitive items. It is incredibly effective—it can permeate almost anything—but it is also toxic, flammable, and painfully slow. A typical EtO cycle can take 1 to 4 hours for exposure, but that is the short part. The real kicker is the aeration period. Because the gas is poisonous, the items must sit in a specialized cabinet for 8 to 12 hours to allow the gas to dissipate safely. As a result: you can't use an EtO-sterilized tool more than once a day. Honestly, it's unclear why more facilities haven't moved away from it faster, except that for some complex materials, nothing else works as well.
Hydrogen Peroxide Gas Plasma: The Fast Alternative
In the 1990s, we saw the rise of Vaporized Hydrogen Peroxide (VHP) and gas plasma systems, like the STERRAD. These are much faster than EtO, with cycles ranging from 28 to 55 minutes. They work by clouding the chamber with peroxide vapor and then "exciting" it with radiofrequency or microwave energy to create a plasma. This process breaks down into water and oxygen, meaning there is no long aeration time. You can use the tools almost immediately. But people don't think about this enough: VHP has strict limitations on lumen length and material compatibility. You can't put cellulose (paper) or certain linens in there because they will "soak up" the peroxide and abort the cycle. It is a trade-off between the speed of the process and the versatility of the load.
Dry Heat and Radiation: The Industrial Outliers
Dry heat sterilization is basically a high-tech pizza oven. It is used primarily for powders, oils, and glassware that steam can't penetrate or might damage. Because air is a poor conductor of heat, the temperatures must be higher—usually 160 to 170 degrees Celsius—and the times are significantly longer. We are talking 60 to 120 minutes of holding time. It is a niche method, largely replaced by steam, yet it remains indispensable for certain pharmaceutical applications where moisture is a deal-breaker. Then there is Gamma Radiation. This is the king of industrial speed for single-use items like syringes or bandages. While the items are exposed to Cobalt-60 for a specific duration, the high-energy photons kill microbes by shattering their DNA instantly. It is incredibly fast for high-volume manufacturing, but the regulatory hurdles and the need for a literal nuclear source make it impossible for hospital use. Which explains why your local clinic still relies on that noisy autoclave in the back room.
Comparing the Clock: Method vs. Duration
To put these differences into perspective, consider the following data points on typical processing windows for common medical devices. A flash sterilization cycle (now officially called "Immediate Use Steam Sterilization" or IUSS) takes about 3 to 10 minutes but is strictly for emergencies. Standard wrapped steam takes 45 to 60 minutes total. VHP takes about 45 minutes. EtO takes 14+ hours. If you're managing a busy surgical schedule, these time discrepancies dictate exactly how many instrument sets you need to buy. If you only have one $50,000 camera and it needs EtO, you're only doing one surgery a day. Speed isn't just about safety; it's the primary driver of hospital economics.
Common pitfalls and the illusion of safety
The dry cycle catastrophe
Most practitioners assume the countdown ends when the buzzer sounds, yet the reality is far more precarious. Drying is not a luxury. If you pull a pack that is even slightly damp, you have just engaged in a phenomenon known as wicking. Bacteria from your hands or the ambient air will use that moisture as a highway to migrate through the wrap and contaminate your supposedly sterile load instantly. Moisture creates a bridge for pathogens. The issue remains that a standard 30-minute sterilization cycle frequently requires an additional 20 to 40 minutes of drying time to ensure the integrity of the barrier. It is frustrating to wait. But rushing this stage renders the entire previous hour of energy consumption completely useless. We see this mistake in dental offices constantly where high turnover is prioritized over physics.
Overloading the chamber floor
Density is the enemy of efficacy. When you cram stainless steel trays together like sardines in a tin, you create cold spots where the steam cannot penetrate. The problem is that steam must displace all air to reach 134 degrees Celsius for the required exposure window. Because air is heavier than steam, it pools in the bottom of an overstuffed autoclave. As a result: the items at the top might be sterile while the items at the bottom are merely warm and dirty. You must leave at least 5 centimeters of space between the chamber walls and your packs. People hate wasting a cycle on a half-empty machine. Let's be clear: a half-sterile load is just a contaminated load with an expensive receipt.
The bio-burden variable and expert calibration
Why cleaning duration dictates killing duration
How long does sterilization take? That depends entirely on how well you scrubbed the forceps ten minutes ago. If you leave a microscopic fragment of organic tissue—blood, bone, or saliva—on a hinge, you have created a physical shield. Steam cannot penetrate a dried blood clot effectively within a standard 4-minute flash cycle. This layer acts as an insulator for the microbes underneath. The issue remains that we often talk about "cycle time" as a fixed mathematical constant, except that it is actually a variable dependent on pre-processing. Expert advice? Use an ultrasonic cleaner for exactly 10 minutes prior to the autoclave to ensure the bio-burden is zero. (Even a tiny fleck of protein can survive 121 degrees if it is buried deep enough). If the surface isn't physically clean, the clock never truly starts ticking for the microbes.
Frequently Asked Questions
Can I speed up the cooling process for faster turnaround?
Forcefully cooling a load by placing it in front of a fan or on a cold stone surface is a recipe for disaster. This rapid temperature drop causes "thermal shock," which can lead to condensation forming inside the sterile pouches. Industry data suggests that cooling should occur in a low-traffic area for at least 30 to 60 minutes. If you touch a warm pack, the pressure from your fingers can actually suck microbes through the paper fibers. The issue remains that rushing the end-phase is the primary cause of internal moisture contamination in 15% of clinical settings. Wait until the packs reach 21 degrees Celsius before storage.
Does the altitude of my facility change the timing?
Physics does not care about your schedule, and atmospheric pressure plays a massive role in how water turns to steam. At higher altitudes, water boils at a lower temperature, which explains why autoclaves must be calibrated to compensate for the lack of external pressure. A cycle in Denver might require a higher PSI of 30 or more to achieve the same internal temperature as a cycle in Miami. Most modern Class B sterilizers use vacuum pumps to bypass this, but older gravity units will fail if not adjusted. You must verify your local boiling point and ensure the machine reaches the saturated steam threshold regardless of your elevation.
How often should we run biological indicators to verify time?
While some regulations suggest weekly testing, experts in high-risk environments advocate for daily biological monitoring. These tests use Geobacillus stearothermophilus spores, which are 10 times more resistant than typical hospital pathogens. If the spores die within your 15-minute cycle at 121 degrees, you have proof of efficacy. Chemical tape only tells you the heat was present, not that the time was sufficient for a total kill. Data from 2024 audits indicates that 8% of autoclaves fail their biological tests despite showing "passed" on the digital display. Consistency is the only metric that matters when human lives are the denominator.
The reality of the terminal kill
We are obsessed with the clock, but the clock is a liar if the parameters of pressure and purity are ignored. It is easy to assume that more time always equals more safety. The problem is that over-processing degrades your expensive instrumentation while under-processing invites litigation and infection. Sterilization is a binary state; there is no such thing as "mostly sterile" in a surgical environment. We must stop asking how we can shave five minutes off the timer and start asking how we can guarantee every second is utilized correctly. As a result: the only responsible approach is to treat the manufacturer guidelines as a floor, not a ceiling. Let's be clear: if you are cutting corners on the 60-minute total turnaround, you aren't being efficient, you are being dangerous. Trust the indicators, respect the physics, and never prioritize the schedule over the science of the kill.