Decoding the True Nature of the Beast: Pathophysiology and Presentation
What Happens When the Arterial Wall Fails
Let us be real here. A pseudoaneurysm is not just a standard bulge; it is an active, ticking clock. When a sheath slips out of the common femoral artery after a percutaneous coronary intervention, blood escapes into the surrounding soft tissue under systemic pressure. But the surrounding fascial planes hold it back, creating a false lumen. The persistent track between the artery and this turbulent pool is the neck. The thing is, this neck behaves entirely unpredictably. I have seen tiny necks clot spontaneously, while others rip wide open under the slightest spike in blood pressure. The fluid mechanics inside the sac are chaotic, featuring a classic "to-and-fro" flow pattern that prevents normal coagulation from sealing the leak.
The Real-World Picture Beyond the Textbook Symptoms
Patients do not just show up with a neat, isolated symptom. They present with a massive, purple, throbbing mass in the groin that makes them scream if you touch it. And people don't think about this enough: the sheer volume of blood trapped in a 6 cm hematoma can mask an absolute free-fall in hemoglobin. You hear a harsh, continuous bruit when you plant your stethoscope over the groin. But if the patient has profound peripheral artery disease, that sound becomes muffled, misleading the junior resident into thinking it is a simple hematoma. That changes everything. If you misdiagnose this as a standard bruise and send them walking, the skin sloughs off within forty-eight hours due to local pressure necrosis.
Navigating the Non-Invasive Frontiers: Compression and Injections
The Brutal Reality of Ultrasound-Guided Compression Repair
Before we go slicing people open, we try to squeeze the leak shut. Ultrasound-guided compression repair looks great on paper. You take the linear probe, find the neck, and push down until the color Doppler signal vanishes. Simple, right? We're far from it. It requires an average of 40 minutes of continuous pressure, which is agonizing for the patient and exhausting for the sonographer. It works best on small tracts under 3.5 cm in patients who are not on aggressive anticoagulation regimens like clopidogrel or enoxaparin. Yet, the failure rate hovers around 30 percent in complex, multi-lobulated sacs, making it an unreliable option for patients who cannot tolerate prolonged pain.
The Game-Changer: Ultrasound-Guided Thrombin Injection
Then came bovine thrombin, and suddenly we had a magic bullet. By injecting a tiny volume of thrombin—usually 500 to 1000 units—directly into the fundus of the pseudoaneurysm, you induce near-instantaneous thrombosis. Which explains why this technique achieved a staggering 96 percent success rate in a famous 2018 registry study out of Cleveland. You must keep the needle tip far away from the neck. Why? Because if even a drop of that enzyme spills into the main femoral stream, you will instantly clot the entire superficial femoral artery, turning a minor groin complication into an emergent surgical catastrophe. Where it gets tricky is when the sac has multiple lobes; do you inject the dominant one or try to hit them all?
When the Scalpel is Unavoidable: Surgical Repair Strategies
Indications for Open Femoral Exploration
Sometimes the needle fails, or the skin is so tense it looks ready to burst. That is when you call the vascular team. Open surgery is mandatory if the pseudoaneurysm exceeds 5 cm, exhibits rapid expansion, or is accompanied by signs of local infection or overlying cutaneous ischemia. Honestly, it's unclear why some centers still try to inject infected sacs, as it almost always leads to mycotic disaster. If the patient is in frank shock with a retroperitoneal hematoma from a high arterial stick, you do not waste time in the ultrasound suite. You move straight to the operating room.
Step-by-Step Surgical Reconstruction Technique
The patient is prepped from umbilicus to mid-thigh. You make a vertical incision directly over the femoral bifurcation, avoiding the mass itself initially to prevent premature rupture. Proximal control is established at the external iliac artery or the very proximal common femoral artery. This is crucial because when you finally cut into the hematoma, the bleeding will be torrential. Once clamps are applied, you evacuate the old, dark clot to expose the arterial defect. The issue remains: the arterial wall around the hole is often shreddy and friable like wet tissue paper. You cannot just throw a simple Prolene stitch into it. You usually need a bovine pericardial patch or a customized Dacron interposition graft to bridge the gap without narrowing the lumen.
Evaluating the Alternatives: Covered Stents versus Surgery
The Endovascular Option for High-Risk Surgical Candidates
What if the patient is ninety years old, has severe heart failure, and a groin that looks like a war zone? You do not want to put them through a full general anesthetic for an open femoral pseudoaneurysm repair. Instead, you opt for an endovascular covered stent graft. By deploying a self-expanding Viabahn stent across the arterial hole, you exclude the pseudoaneurysm sac immediately from the circulation. It is an elegant fix. But it comes with a heavy price: you are placing a permanent piece of metal right across the hip joint line, a zone of constant flexion. Experts disagree on the long-term patency of these stents, with some studies showing a 15 percent occlusion rate within two years due to stent fracture or intimal hyperplasia. As a result: we reserve this strictly for those who might not survive the knife.
Common mistakes and dangerous misconceptions
The compression blind spot
Many clinicians assume manual compression is a foolproof, benign starting point for every single iatrogenic vascular injury. Let's be clear: blindly pressing on a groin without mapping the exact anatomical neck of the lesion is a recipe for cutaneous necrosis. You cannot compress what you cannot see. The problem is that prolonged, aggressive force frequently obliterates the adjacent femoral vein instead of sealing the arterial hole. This oversight causes acute deep vein thrombosis, an entirely preventable catastrophe that complicates the patient's recovery trajectory. Is it really worth risking a massive pulmonary embolism just because you wanted to avoid a minor percutaneous intervention?
Misjudging the true cavity size
Ultrasound can lie to you if your settings are wrong. Practitioners frequently misinterpret the hypoechoic swirl of a femoral pseudoaneurysm, confusing a massive, multi-lobulated sac for a small, easily manageable cavity. Why does this happen? Sluggish, partially thrombosed peripheral zones often blend into surrounding hematomas on low-frequency transducers, which explains why operators sometimes under-inject thrombin. They target only the patent core. Consequently, the remaining unstable sac continues to expand under systemic pressure, leading to delayed rupture twenty-four hours later. Except that a secondary rupture into the retroperitoneal space carries a mortality rate exceeding 15% in frail patients.
Advanced expert strategies and the dual-lumen trick
Simultaneous balloon occlusion
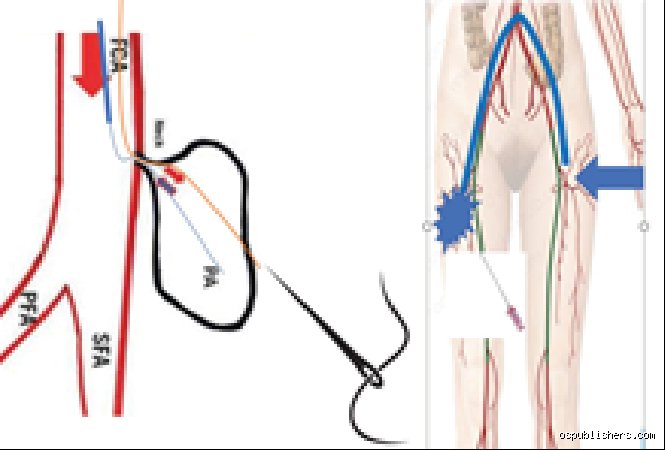
When you attempt to repair a femoral pseudoaneurysm via ultrasound-guided thrombin injection, the terrifying phantom in the room is systemic embolization. If that bovine enzyme escapes into the native circulation, you are suddenly treating an acute, limb-threatening ischemic event. To mitigate this nightmare, elite interventionalists utilize a temporary contralateral crossover balloon. By inflating a compliant balloon at 4 French directly across the arterial defect, you create an impenetrable mechanical barrier. As a result: the thrombin stays exactly where it belongs, polymerizing the turbulent sac while the native femoral flow is completely protected. Yet, this elegant maneuvers requires superb fluoroscopic dexterity and an extra arterial access site.
Navigating the short-neck dilemma
A neck shorter than 2 millimeters usually disqualifies a patient from standard percutaneous sealing techniques. However, we have found that utilizing a highly viscous, micro-fibrillar collagen paste alongside a microballoon can successfully bridge this anatomical deficit. It requires supreme patience. You must hold the balloon inflated for exactly 180 seconds while the matrix solidifies against the external arterial wall, an agonizingly long time when a patient is squirming on the table (usually due to inadequate local anesthesia). But this advanced method saves the patient from an emergency open surgical exploration under general anesthesia.
Frequently Asked Questions
What is the definitive success rate of ultrasound-guided thrombin injection?
Large-scale clinical registries indicate that ultrasound-guided thrombin injection boasts a primary success rate between 92% and 97% for uncomplicated lesions. However, this impressive number drops significantly to roughly 72% when managing patients concurrently receiving dual antiplatelet therapy or continuous systemic heparin infusions. Recurrence in these anticoagulated individuals often manifests within 48 hours, requiring either a secondary injection or a definitive transition to covered stent placement. Operators must achieve a thrombin concentration of at least 1,000 units per milliliter to guarantee rapid stagnation of flow within high-velocity tracts.
How do you manage an infection after a percutaneous repair attempt?
An infected false aneurysm is an absolute surgical emergency that completely precludes any further endovascular or percutaneous intervention. The issue remains that introducing thrombin or deploying a covered stent into an active bacteremic field triggers rapid graft infection and catastrophic arterial wall dissolution. Broad-spectrum intravenous antibiotics must be initiated immediately, followed by urgent open surgical excision of the infected sac, aggressive local debridement, and autologous vein patch angioplasty using the great saphenous vein. Attempting conservative management in this scenario is a fatal error, as femoral artery disruption from mycotic erosion carries an amputation risk of nearly 30%.
When must an operator abandon endovascular techniques for open surgery?
You must abandon percutaneous approaches immediately if the patient develops skin ischemia, rapidly expanding groin ecchymosis, or severe neurological deficits stemming from femoral nerve compression. Furthermore, persistent flow after two separate, technically sound thrombin injection attempts indicates a structural failure that endovascular tools cannot safely fix. A widening retroperitoneal hematoma accompanied by a sudden drop in systolic blood pressure below 90 millimeters of mercury demands an immediate transition to the operating theater. In short, your ego must never dictate the clinical timeline when a patient is actively exsanguinating into their pelvis.
A definitive paradigm shift in vascular preservation
The historical obsession with immediate open surgical ligation for every vascular complication is an outdated relic that modern medicine must aggressively discard. We must treat the repair a femoral pseudoaneurysm not as a routine checkbox task, but as a nuanced exercise in precise hemodynamic control. Relying solely on blind manual pressure is a lazy, hazardous practice that unnecessarily compromises patient safety and prolongs hospital stays. Ultrasound-guided interventions, reinforced by temporary balloon occlusion when necessary, represent the absolute gold standard of care. Our collective clinical objective must shift completely away from reactionary crisis management toward early, proactive, image-guided exclusion. Ultimately, protecting native arterial integrity through minimalist, precise endovascular techniques is the only acceptable standard for modern vascular specialists.