The Anatomy of a Catastrophe: Why Vessels Fail and What Happens if Aneurysm Bursts
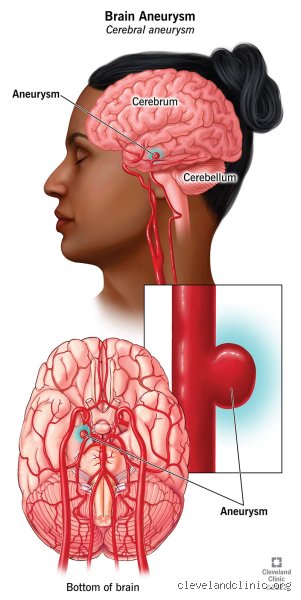
Think of your cerebral arteries as a high-pressure plumbing system built out of delicate, living tissue that never gets a day off. Most of the time, these vessels are remarkably resilient, but occasionally, a structural "soft spot" develops—usually at a bifurcation or a sharp turn where hemodynamic stress is at its peak—and the wall begins to pouch out like a cheap tire about to blow. We call this an aneurysm, and for many, it sits there for decades, doing absolutely nothing, just a silent passenger in the circle of Willis. Yet, when the structural integrity finally gives way, the transition from a stable state to a life-threatening crisis happens in milliseconds. The thing is, we still don't fully understand why some tiny 3mm blebs stay quiet while others decide to ruin a Tuesday afternoon without warning.
The Physics of the Blowout
The moment the wall tears, arterial blood, which is under significant pressure from the heart's constant pumping, jets into the subarachnoid space. This isn't a slow leak. Because the brain is encased in a rigid skull, there is nowhere for this extra fluid to go, leading to an immediate and dangerous spike in intracranial pressure. Imagine trying to force an extra quart of water into a sealed, non-expandable ceramic jar that is already full; something has to give, and in this case, it is the delicate neural tissue being crushed against the bone. Does it hurt? Beyond what most humans can conceptualize. This sudden pressure surge can actually stop blood flow to the rest of the brain entirely for a few seconds, which explains why so many victims drop to the ground instantly.
The Genetic and Lifestyle Hand
While some point to pure bad luck, there are clear markers that heighten the stakes, specifically Polycystic Kidney Disease (PKD) and Ehlers-Danlos syndrome, which weaken connective tissues throughout the body. But honestly, it's unclear why two people with the same blood pressure and the same smoking habits have such wildly different outcomes. I've seen lifelong smokers with pristine arteries and athletes with saccular aneurysms the size of a grape. It feels like a rigged game of biological roulette. Yet, we cannot ignore that chronic hypertension remains the primary driver of wall degradation over time, acting like a constant hammer against a thinning nail.
The Cascade of Neurological Chaos: From First Tear to Total System Failure
When we talk about what happens if aneurysm bursts, we are really talking about a domino effect of cellular death that begins the second the blood touches the brain. Blood is supposed to stay inside the pipes; when it escapes, it becomes incredibly toxic to neurons. The iron and other breakdown products in the blood cause vasospasm, where nearby healthy arteries constrict in a misguided attempt to stop the bleeding, effectively starving the rest of the brain of oxygen. This secondary ischemia can be even more damaging than the initial bleed. It’s a cruel irony of human biology—the body’s defense mechanism against bleeding out ends up causing a massive stroke by cutting off its own supply lines.
The Thunderclap Headache and Symptom Progression
The hallmark of a rupture is the "worst headache of your life," a pain so visceral that patients often describe it as being struck by a physical object. But that changes everything when the secondary symptoms kick in, such as photophobia, a stiff neck (nuchal rigidity), and cranial nerve palsies that might make one eye droop or go out of alignment. If the bleed is located near the posterior communicating artery, for instance, the third cranial nerve gets compressed almost immediately. People don't think about this enough, but the location of the bulge dictates the specific flavor of the disaster. A burst in the anterior communicating artery might cause personality shifts or lower limb weakness, whereas a basilar artery rupture is frequently and tragically terminal before the ambulance even arrives.
Chemical Warfare in the Skull
As the blood begins to clot and then break down, it releases inflammatory mediators that irritate the meninges, the brain's protective lining. This causes the fever and extreme neck pain that often mimics meningitis, leading to occasional, and sometimes fatal, misdiagnoses in overcrowded ERs. Around day three to five, the risk of vasospasm peaks, which is why patients are kept in the ICU for at least two weeks post-rupture. We're far from it being a "fix it and forget it" surgery; the post-operative window is a minefield of delayed cerebral ischemia and hydrocephalus. The issue remains that even a "successful" clipping or coiling doesn't mean the brain is out of the woods, as the chemical environment remains hostile for days.
Immediate Physiological Response: Why the Body Shuts Down
The autonomic nervous system goes into an absolute frenzy the moment the rupture occurs. You see a massive release of catecholamines—essentially a "sympathetic storm"—which can cause the heart to mimic a heart attack, a phenomenon known as neurogenic stunned myocardium. It is a total systemic meltdown. Because the brain is the command center, its distress signal throws every other organ into a panic. As a result: the lungs may fill with fluid (pulmonary edema) and the heart rate may plummet or spike erratically. Experts disagree on whether this is a protective hibernation attempt or just the "blue screen of death" for the human operating system, but regardless, it makes the task of the neurosurgeon infinitely more complex.
The Cushing Triad and Intracranial Pressure
Clinical teams look for the Cushing Triad—bradycardia, irregular respirations, and a widening pulse pressure—as a sign that the brain is about to herniate. This is the point of no return where the brain is literally pushed down through the foramen magnum at the base of the skull because the pressure is so high. It is a grisly, mechanical end to a biological problem. But if caught before this stage, external ventricular drains can be inserted to diverted cerebrospinal fluid and blood, relieving the pressure just enough to perform more definitive repairs. Which explains why every second counts; a delay of ten minutes can be the difference between walking out of the hospital and a lifetime in a vegetative state.
Risk Assessment: Aneurysm Rupture vs. Other Cerebrovascular Events
It is easy to confuse a ruptured aneurysm with a standard ischemic stroke or a simple migraine, except that the onset is radically different. Ischemic strokes usually involve a gradual "fading out" of function—a numb arm, a slurred word—whereas a rupture is an explosion. In 2024, a high-profile case in London involved a 42-year-old marathon runner who collapsed mid-stride; bystanders assumed it was cardiac arrest, but it was a berry aneurysm that had been lurking since birth. This highlights the terrifying randomness of the condition. While a transient ischemic attack (TIA) acts as a warning shot, a burst aneurysm offers no such courtesy; it is the final act, not the rehearsal.
Comparing Clipping and Coiling Outcomes
The medical community has shifted significantly toward endovascular coiling over the last two decades, largely because it doesn't involve sawing through the cranium. Yet, the nuance lies in the recurrence rates, which are slightly higher with coiling than with the traditional microvascular clipping. If you are 30 years old, you might want the permanent security of a titanium clip, even if the recovery is more brutal, whereas an 80-year-old might not survive the open surgery. Where it gets tricky is when the aneurysm is "wide-necked," making coiling nearly impossible without a stent, which then requires long-term blood thinners—a dangerous prospect if you've just had a brain bleed. It's a constant balancing act of risks that doctors have to navigate in the heat of a crisis.
Common misconceptions and the "migraine" trap
The silence before the storm
Many assume a cerebral hemorrhage provides a polite warning, perhaps a dull ache or a flickering vision that lingers for weeks. Let's be clear: vascular catastrophes are rarely so considerate. A common mistake involves dismissing the "thunderclap headache" as a mere tension migraine because the person has a history of sinus issues. Except that a standard migraine builds like a slow tide, whereas a ruptured aneurysm hits like a physical blow from a hammer. Because the brain tissue is being inundated with pressurized blood, the sensation is instantaneous. Data indicates that nearly 25% of patients are initially misdiagnosed when they present with "minor" leaks, often called sentinel bleeds. This is a lethal oversight. The problem is that we treat the brain as a resilient organ when, in reality, it is a delicate jelly encased in a rigid vault. If you feel the worst pain of your life, do not reach for ibuprofen.
The myth of the elderly victim
We often visualize stroke-like events as the exclusive domain of the octogenarian. This is a dangerous fallacy. While age increases risk, saccular aneurysms frequently rupture in individuals aged 35 to 60. In fact, statistics show that women are 1.5 times more likely to develop these "berry" protrusions than men. Why do we ignore this? Perhaps it is our collective denial regarding our own fragility. It remains a staggering reality that a seemingly fit 40-year-old can harbor a ticking time bomb in the Circle of Willis without a single clinical symptom until the moment of catastrophe. The issue remains that screening is not a standard protocol for the general population, which explains why the first sign of trouble is often the last.
The vasospasm: The hidden secondary killer
The toxic aftermath of blood
Survival of the initial burst is only the first hurdle in the race against the clock. Imagine the initial rupture is a fire; the vasospasm is the subsequent structural collapse that happens days later. When an aneurysm bursts, the subarachnoid space fills with blood that eventually breaks down, releasing irritating byproducts. These chemicals cause nearby arteries to shrink and tighten. As a result: the brain suffers from a secondary "delayed" stroke because it is being starved of oxygenated blood. This typically occurs between day 4 and day 12 post-rupture. We monitor this using Transcranial Doppler (TCD) ultrasounds to measure flow velocity. Yet, even with modern nimodipine treatments, approximately 30% of survivors face some degree of permanent neurological deficit from this secondary narrowing. (It is a cruel irony that the very blood meant to nourish the brain becomes the poison that strangulates it.) Can we ever truly predict who will suffer the most? Currently, our predictive models are far from perfect, which is a humbling admission for modern medicine.
Frequently Asked Questions
What are the actual survival rates after a rupture?
The numbers are sobering and reflect the extreme gravity of a subarachnoid hemorrhage. Historically, approximately 40% of cases result in immediate or near-immediate mortality before the patient even reaches a surgical suite. For those who do make it to the hospital, the prognosis depends heavily on the Hunt and Hess scale grade at the time of admission. Around 66% of survivors will suffer some form of long-term neurological impairment, ranging from cognitive shifts to physical paralysis. In short, the window for intervention is narrow, and the statistical reality favors those who receive endovascular coiling or surgical clipping within the first 24 hours.
Does a family history guarantee I will have one?
Genetics certainly play a role, but they are not a guaranteed sentence of doom. If you have two or more first-degree relatives who have suffered a ruptured brain aneurysm, your personal risk increases by approximately 10% to 15%. This justifies proactive MRA or CT angiography scans to look for unruptured lesions. But most cases are sporadic rather than purely hereditary. Smoking remains the single most aggressive modifiable risk factor, increasing the likelihood of a rupture by nearly 300% compared to non-smokers. Consequently, your lifestyle choices often shout louder than your DNA when it comes to vascular integrity.
How long is the recovery process for survivors?
Recovery is not a linear path but a grueling marathon that spans months or even years. The brain requires immense time to reabsorb the extravasated blood and heal the localized trauma caused by the intracranial pressure spike. Most intensive rehabilitation happens in the first 6 months, during which physical and occupational therapy are used to rewire neural pathways. Many patients struggle with "invisible" symptoms like profound fatigue, mood swings, and short-term memory loss that do not show up on a scan. Patients often report that the emotional trauma of surviving a near-death event is just as taxing as the physical healing of the vessel itself.
The radical necessity of immediate action
We must stop treating "sudden headaches" as inconveniences and start treating them as potential neurosurgical emergencies. Our culture of "toughing it out" is fundamentally incompatible with a ruptured aneurysm. To wait is to invite a permanent darkness that no amount of late-stage surgery can fully reverse. If the sylvian fissure is flooded with blood, every second spent debating an ER visit is a second of brain tissue lost to ischemia. We must demand a healthcare shift toward faster triage for neurological pain. It is better to have a negative CT scan and a bruised ego than a positive autopsy. Let's be clear: your life is worth the perceived "drama" of an emergency call. The issue remains that we only value our vascular health once it has already failed us.