Understanding the Pathology: Where it Gets Tricky for Modern Clinicians
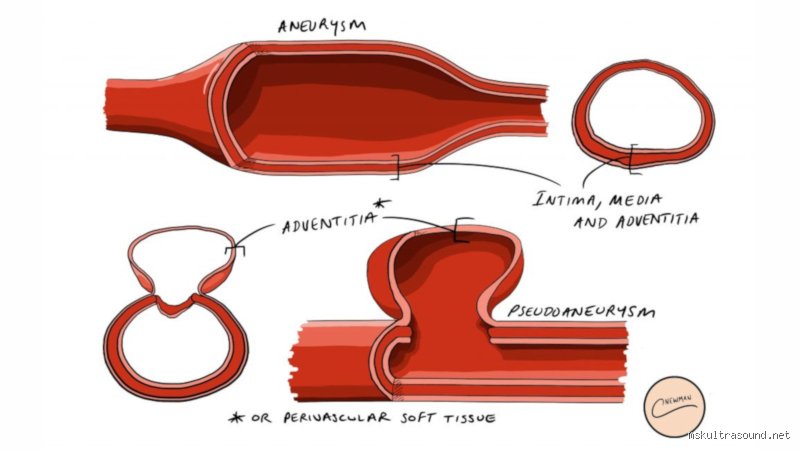
The issue remains that the term pseudoaneurysm—often called a "false aneurysm"—is frequently thrown around in imaging reports without sufficient respect for its volatile nature. Unlike a true aneurysm, which involves all three layers of the arterial wall (intima, media, and adventitia), a pseudoaneurysm occurs when a hole in the arterial wall allows blood to escape and form a pressurized pocket. This pocket is only held back by a thin, fragile layer of thrombus or overlying soft tissue. I firmly believe that the "giant" label is more than just a measurement; it is a warning of impending mechanical failure. But how do we decide when a collection moves from "moderate" to "giant" status? The traditional 5-centimeter rule originated largely from femoral artery studies following cardiac catheterization procedures in the 1990s, yet its application across the carotid or visceral arteries is often debated by specialists today.
The Anatomy of a Contained Catastrophe
When blood exits the vessel under high pressure, it carves out a cavity in the surrounding muscle or fat. Because this cavity lacks the structural integrity of an actual blood vessel, the risk of spontaneous rupture increases exponentially as the radius of the sac expands. Physics dictates this through the Law of Laplace, where the wall tension is proportional to the radius; hence, a giant pseudoaneurysm faces forces that smaller ones simply do not. Is it any wonder these structures can grow to the size of a grapefruit in a matter of days if left unchecked? And because the "wall" of the sac is nothing more than compressed fibrin and clotted blood, it offers almost zero resistance to the relentless hammering of the systolic pulse. That changes everything when you are planning a repair, as you aren't suturing healthy tissue, but rather managing a blowout in a pile of disorganized debris.
The 5-Centimeter Benchmark: Navigating the Metrics of a Giant Pseudoaneurysm
If we look at the data from the Mayo Clinic or the Society for Vascular Surgery, the consensus for the femoral region—the most common site for these lesions—consistently points toward the 50 mm threshold as the definition of "giant." Yet, there is a catch. A 4-centimeter pseudoaneurysm in the neck, specifically involving the carotid artery, is often treated with the same urgency as a 10-centimeter one in the thigh because the consequences of a "minor" rupture in the cervical space involve immediate airway compression or stroke. In short, the definition is as much about the neighborhood as it is about the house. Clinical studies from 2021 suggest that giant pseudoaneurysms of the visceral arteries, such as the splenic or hepatic arteries, are exceedingly rare but carry a mortality rate exceeding 25 percent if they exceed 5 centimeters before discovery. We're far from a one-size-fits-all metric, but the 5-centimeter mark remains the most reliable red flag in a radiologist's toolkit.
Variations in Diameter Across Anatomical Sites
In the radial artery, even a 2-centimeter collection could be considered "giant" relative to the local anatomy. Because the wrist has so little room for expansion, a pseudoaneurysm there causes nerve compression and skin necrosis long before it reaches the 5-centimeter mark favored by the textbooks. Which explains why some surgeons are pushing for a more proportional definition of "giant" that accounts for the parent vessel's diameter. Except that the medical coding and standardized reporting systems still demand hard numbers. In a large-scale retrospective review of 450 patients conducted at a major European trauma center between 2018 and 2023, pseudoaneurysms classified as giant (mean size 6.4 cm) were three times more likely to require open surgical intervention rather than the less invasive ultrasound-guided thrombin injection. This data suggests that once you cross that 5-centimeter threshold, the success rate of non-surgical techniques plummets.
Growth Velocity and the Giant Label
The speed of expansion is a factor experts disagree on, honestly, it's unclear if a slow-growing 5-centimeter sac is as dangerous as a 3-centimeter one that appeared overnight. A rapidly expanding hematoma creates a massive inflammatory response in the surrounding tissues. This inflammation obscures surgical planes and makes the eventual repair—whether endovascular or open—a technical nightmare (and believe me, you don't want to be the resident trying to find the "neck" of the aneurysm in a sea of inflamed tissue). As a result: many trauma surgeons now use the term giant to describe any pseudoaneurysm that is symptomatic, regardless of whether it hit the 50 mm mark. But for the sake of scientific rigor, we stick to the 5 cm rule to ensure we are comparing apples to apples in the literature.
Clinical Presentation and the Physical Reality of Massive False Aneurysms
A giant pseudoaneurysm is rarely a silent neighbor. You can usually feel it. It presents as a pulsatile mass, often accompanied by a distinct "bruit" or whooshing sound that can be heard with a stethoscope. But the thing is, as these masses grow, they begin to compress everything in their path. A giant femoral pseudoaneurysm doesn't just threaten to bleed; it pinches the femoral nerve, leading to excruciating leg pain and weakness, and it can obstruct the adjacent femoral vein, causing massive leg swelling that mimics a deep vein thrombosis. This is where the diagnosis gets messy. Because the symptoms overlap so heavily with other vascular conditions, a physical exam alone is never enough. We rely on Color Doppler Ultrasound and CT Angiography to provide the precise measurements needed to confirm if we are dealing with a giant-scale problem or something more manageable.
Complications Specific to the "Giant" Classification
The most terrifying complication of a giant pseudoaneurysm is integumentary compromise—essentially, the pressure from the blood sac is so high that it cuts off the blood supply to the overlying skin. When the skin starts to turn dusky or purple, you are looking at an imminent external rupture. This is a surgical emergency of the highest order. Data indicates that pseudoaneurysms over 6 centimeters have a skin necrosis rate of roughly 12 percent, a statistic that should keep any vascular fellow up at night. Furthermore, large sacs often contain significant amounts of mural thrombus. This old, clotted blood can break loose and travel downstream, causing distal embolization and acute limb-threatening ischemia. It is a cruel irony: the body's attempt to clot off the leak actually creates the seeds for a potential amputation.
Comparing Giant Pseudoaneurysms to True Aneurysmal Dilations
While a giant abdominal aortic aneurysm (AAA) is a well-known entity, a giant pseudoaneurysm is a different beast entirely. A 5-centimeter AAA might be monitored for years with a "wait and see" approach, provided it isn't growing too fast. But a 5-centimeter pseudoaneurysm? You don't watch that. You fix it. The structural instability is simply too high. Where it gets tricky is explaining this to patients who have heard that "5 centimeters is the cutoff for surgery" in other contexts. In the case of a pseudoaneurysm, the wall is essentially made of tissue paper and hope, whereas a true aneurysm still has some leftover structural proteins from the original vessel wall. This distinction is the primary reason why the management of giant pseudoaneurysms is almost always aggressive. There is no such thing as a "stable" giant pseudoaneurysm; there are only those that haven't ruptured yet.
Diagnostic Nuances in Large-Scale Imaging
On a CT scan, a giant pseudoaneurysm often presents with the "yin-yang sign" on ultrasound, representing the turbulent swirl of blood entering and exiting the sac. But on a Contrast-Enhanced CT, the giant variety can look like a massive, disorganized tumor if the radiologist isn't careful. The key is identifying the "neck"—the narrow channel connecting the artery to the sac. In giant cases, the neck can be quite wide, sometimes exceeding 1 centimeter in diameter, which makes simple treatments like thrombin injection much riskier, as the medicine can leak back into the main artery and cause a massive stroke or limb loss. This technical detail is exactly why size is the primary determinant of the treatment algorithm. As we transition into discussing the specific management strategies for these behemoths, we must remember that every millimeter of the sac represents millions of red blood cells waiting for a way out.
The Pitfalls of Perception: Common Misconceptions
The medical community often stumbles over the threshold of anatomical scale because we treat diagnostic guidelines like immutable laws. The problem is that many clinicians assume a giant pseudoaneurysm must present as a visible, pulsating mass to earn its terrifying title. It is a lie. Deep-seated pelvic or visceral lesions can exceed 8 centimeters while remaining clinically silent until they achieve catastrophic rupture. Size is a relative metric of disaster. Because of this, assuming that a small skin surface protrusion equates to a minor internal hematoma is a recipe for surgical regret. We see this often in post-catheterization complications where a 2-centimeter superficial bulge masks a massive, 10-centimeter deep-tissue collection.
Measurement Inconsistency
Radiologists sometimes differ on whether to measure the outer-to-outer diameter or merely the blood-filled lumen. Let's be clear: the external dimensions of the surrounding thrombus define the mass effect, yet the internal flow dictates the rupture risk profile. If you ignore the wall thickness, you are miscalculating the true spatial footprint of the pathology. A 5-centimeter cavity surrounded by 3 centimeters of organized clot is effectively an 8-centimeter ticking bomb. Which explains why a unified measurement protocol remains elusive in many trauma centers today.
The "Safe" Threshold Myth
Do you really think a 4.9-centimeter lesion is safe while a 5.1-centimeter one is a crisis? Biology does not respect our decimal points. The issue remains that hemodynamic instability can occur at any size if the arterial neck is wide enough to facilitate high-velocity jetting. A "smaller" 4-centimeter femoral lesion with a 1,200 mL/min flow rate is far more lethal than a 6-centimeter sluggish one. As a result: fixation on the "giant" label can distract you from the kinetic energy contained within the sac. Irony dictates that the largest masses are sometimes the most stable because they have already reached a pressure equilibrium with the surrounding compartment.
The Ghost in the Machine: Hemodynamic Sequestration
There is a clandestine reality to the giant pseudoaneurysm that textbooks rarely whisper about: it acts as a secondary heart. When a lesion surpasses the 100-millimeter mark, it starts sequestering a significant percentage of the total stroke volume. This is not just a hole in a pipe; it is a parasitic chamber. But practitioners often forget to check for high-output cardiac failure in these patients. The heart is working overtime to fill a dead-end void that offers zero systemic perfusion. It is an exhausting, futile physiological loop. (This is especially true in renal or splenic artery cases where the visceral flow is already high.)
Turbulence and Thrombin Consumption
Within these massive architectural failures, the blood does not simply sit still. It swirls in violent, chaotic eddies that destroy platelets on contact. In short, a sufficiently massive false aneurysm can induce a localized consumptive coagulopathy. You aren't just treating a vascular bulge; you are fighting a miniature war against the patient’s own clotting factors. If the diameter exceeds 12 centimeters, the surface area for fibrinogen depletion becomes immense. Yet, we rarely see surgeons order a full coagulation panel before addressing the mechanical repair, which is a dangerous oversight in the operating theater.
Frequently Asked Questions
Is there a specific diameter that defines a giant pseudoaneurysm?
While the literature is somewhat fractured, the consensus threshold for the "giant" designation typically begins at 50 millimeters, though some high-volume centers push this to 80 millimeters for aortic variants. Data from a 2022 retrospective study showed that lesions exceeding 5 centimeters have a spontaneous rupture rate exceeding 40 percent without intervention. These dimensions are not arbitrary because they correlate with the failure of the surrounding adventitia or hematoma wall to contain systolic pressure. Small lesions under 2 centimeters might resolve with ultrasound-guided compression, but once you cross the 5-centimeter mark, the physics of wall tension shifts dramatically. The Laplace law dictates that as the radius increases, the tension on the wall grows exponentially, making 50 millimeters a logical tipping point.
Can a giant pseudoaneurysm exist without any pain?
Pain is an unreliable narrator in vascular medicine. Patients with significant adipose tissue or deep-seated iliac lesions can harbor a 7-centimeter giant pseudoaneurysm for months without feeling anything more than a vague bloating. The issue remains that the retroperitoneum can accommodate a massive amount of fluid—up to 4 liters—before internal pressure triggers the sensory nerves. By the time the patient presents with acute discomfort, the lesion has often already compromised the perfusion of distal limbs or adjacent organs. Relying on subjective symptoms rather than objective imaging like CTA or Duplex ultrasound is a gamble with the patient's life. We must prioritize aggressive screening in post-surgical patients regardless of their pain levels.
What are the primary risks of leaving a large lesion untreated?
The most immediate threat is catastrophic hemorrhage, but the secondary risks are equally grim, including distal embolization and skin necrosis. As the thrombus inside the sac becomes unstable, fragments can break off and travel downstream, potentially causing limb-threatening ischemia or "blue toe syndrome." Furthermore, the sheer physical bulk of an 8-centimeter mass can compress adjacent veins, leading to deep vein thrombosis or agonizing nerve palsies. Statistics indicate that untreated lesions over 6 centimeters have a 60 percent complication rate within the first 30 days of detection. Except that many people think "watchful waiting" is an option, which is rarely true when dealing with arterial pressures. Surgical or endovascular intervention is the only definitive way to halt the progression of these vascular anomalies.
The Final Verdict on Vascular Scale
The obsession with defining exactly what size a giant pseudoaneurysm is misses the forest for the trees. We must stop worshiping the ruler and start respecting the hemodynamic velocity and the anatomical neighborhood. Let's be clear: any false aneurysm that forces a clinician to change their surgical approach due to its sheer volume is, for all intents and purposes, giant. We admit our limits in predicting exactly when a wall will give way, but the risk-to-benefit ratio of intervention always favors action once the 50-millimeter line is crossed. It is a biological predator that requires aggressive exclusion via stenting or open repair. Do not wait for the "giant" to wake up. By then, the patient's physiological reserves have usually already left the building.