For decades, the conversation surrounding prostate health was whispered in hushed tones, usually involving a terrifyingly large incision and a weeks-long hospital stay that felt more like a sentence than a solution. We are far from that era now. Today, the landscape of urological oncology is being terraformed by artificial intelligence and micro-robotics, making the term surgery almost feel like a misnomer. Because when a surgeon operates through a single 2.5-centimeter incision using a da Vinci SP system, the trauma to the abdominal wall is so negligible that patients are often home by dinner. But does that mean every new bell and whistle is a guaranteed win? Honestly, it’s unclear in some cases, as the "newest" isn't always synonymous with "best" for every specific anatomy. I believe we have reached a tipping point where the surgeon's ego must take a backseat to the data-driven algorithms guiding their hands.
Beyond the Open Incision: Defining the Modern Era of Urological Intervention
To understand where we are, we have to look at the wreckage of where we were. Traditional open surgery, or radical retropubic prostatectomy, required a massive vertical opening below the navel, leading to significant blood loss and a recovery period that could sideline a man for months. It was a blunt instrument approach in a delicate ecosystem. Yet, the shift to laparoscopy in the early 2000s was only a half-step forward because the rigid instruments lacked the "wristed" dexterity needed to navigate the narrow confines of the male pelvis. This is where it gets tricky for the patient trying to do their own research online.
The Rise of Robotic Dominance and the 10,000-Hour Rule
The current standard of care is the Robotic-Assisted Laparoscopic Prostatectomy (RALP). It is not a robot performing surgery; rather, it is a sophisticated tele-manipulator that filters out a surgeon's natural tremors and provides a 3D high-definition view magnified up to ten times. In 2024, approximately 85 percent of prostatectomies in the United States were performed robotically. Experts disagree on whether the robot itself improves cancer-specific survival compared to a master open surgeon, but the data on post-operative pain and blood loss is undeniable. A 2025 study from the Cleveland Clinic indicated that robotic patients required 60 percent less opioid pain medication than those undergoing traditional methods. And yet, the tool is only as good as the person behind the console. You wouldn't want a pilot who has only flown a Cessna to take the controls of a Boeing 787, would you?
Single-Port Technology: The "One Hole" Revolution
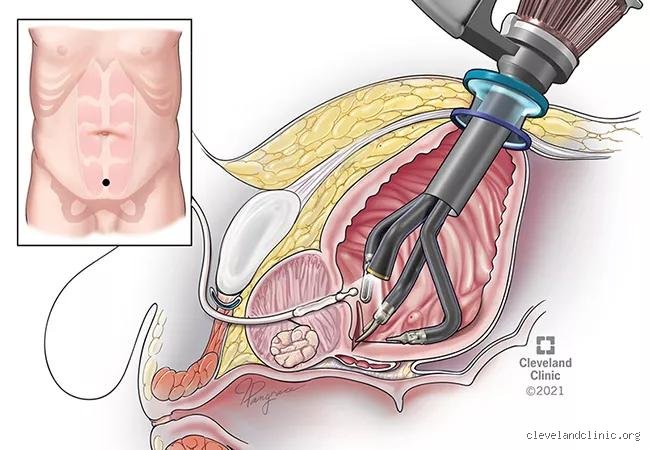
The most recent leap is the Single-Port (SP) robotic platform. Unlike the standard Xi model that requires four or five small incisions across the abdomen, the SP system funnels all instruments—the camera and three working arms—through one single trocar. This allows surgeons to use a transperitoneal or an even more advanced extraperitoneal approach, which avoids entering the bowel cavity entirely. By staying outside the peritoneum, the risk of postoperative ileus—a painful temporary paralysis of the intestines—is virtually eliminated. It’s a game-changer for men with extensive prior abdominal surgeries who were previously told they weren't candidates for minimally invasive work.
The Technical Architecture of Nerve-Sparing and Functional Outcomes
What is the new procedure for prostate surgery if it doesn't protect what matters most? The real technical "magic" isn't just removing the adenocarcinoma; it is the meticulous dissection of the neurovascular bundles. These microscopic threads of nerves, responsible for erections, hug the prostate like a delicate web. In the past, they were often sacrificed "just to be safe." Modern intraoperative frozen sectioning, like the NeuroSAFE technique developed in Hamburg, Germany, allows pathologists to check the margins of the prostate while the patient is still on the table. If the margin is clear, the nerves are saved. If not, only then is the nerve removed. This real-time feedback loop is the difference between a lifetime of medication and a return to normalcy.
The Retzius-Sparing Approach: A Shift in Anatomy
Wait, there is an even more specialized method gaining traction called the Retzius-sparing (Bocciardi) technique. Traditionally, surgeons approach the prostate from the front, cutting through the Retzius space and dropping the bladder, which can disrupt the ligaments supporting the urethral sphincter. The Retzius-sparing method approaches from "behind" the bladder. As a result: the natural support structures of the bladder remain untouched. Early clinical trials show that 90 percent of patients are continent immediately upon catheter removal, a statistic that was unheard of a decade ago. It is technically demanding, which explains why only a fraction of high-volume centers currently offer it.
Indocyanine Green (ICG) and Real-Time Bio-Imaging
We are also seeing the integration of Firefly technology, which uses indocyanine green dye injected into the bloodstream. Under near-infrared light, the blood supply to the prostate and the surrounding lymph nodes glows a vivid neon green. This allows the surgeon to distinguish between healthy tissue and the sentinel lymph nodes that are most likely to harbor metastatic cells. It’s like having a GPS for cancer that highlights the exact path the disease might take to escape. Because we can now see the vasculature with such clarity, we can ensure the bladder neck receives enough blood to heal properly, reducing the risk of anastomotic leaks or strictures.
Focal Therapy: The Middle Ground Between Active Surveillance and Surgery
Not every man needs his entire prostate removed. This is the nuance that many traditionalists still struggle with. For men with intermediate-risk localized prostate cancer, we are seeing the rise of focal therapy, which treats only the tumor and a small "safety margin" of healthy tissue. Think of it like a lumpectomy for the prostate instead of a mastectomy. This changes everything for the patient who is terrified of side effects but can't stomach the anxiety of active surveillance.
TULSA-PRO: Transurethral Ultrasound Ablation
The TULSA-PRO procedure is a fascinating piece of engineering that uses directional ultrasound to "cook" the cancerous tissue from the inside out. The patient is placed inside an MRI scanner, and a device is inserted into the urethra. The MRI provides real-time thermal mapping, ensuring the prostatic capsule stays cool while the tumor reaches lethal temperatures. It’s a bloodless, incision-free afternoon. But here is the catch: because the prostate remains in the body, PSA monitoring remains complex, and long-term 10-year data is still being gathered. People don't think about this enough when they are seduced by the "no-cut" marketing—you are trading an immediate surgical solution for a lifetime of vigilant monitoring.
High-Intensity Focused Ultrasound (HIFU) and Irreversible Electroporation
Then there is HIFU, which uses sound waves focused to a point (much like a magnifying glass with sunlight) to destroy tissue. Or NanoKnife, which uses irreversible electroporation—high-voltage electrical pulses that punch holes in the cell membranes of the cancer, causing them to die without using heat. This is particularly useful for tumors located right next to the rectal wall or the urethral sphincter, where heat-based treatments might cause "collateral" burns. In short, the tool kit is expanding, but the complexity of choosing the right tool has never been higher.
Comparing Modern Robotics with Emergent Non-Invasive Alternatives
When weighing the robotic radical prostatectomy against focal therapies, the decision tree often comes down to cancer control versus side-effect profile. Surgery provides a definitive pathology report—you know exactly what was in there once it's under the microscope. Focal therapies rely on the accuracy of multiparametric MRI and fusion biopsies, which, while excellent, can occasionally miss secondary "satellite" lesions. As a result: about 20 to 25 percent of focal therapy patients may eventually require a "salvage" prostatectomy if the cancer recurs or was underestimated.
The Cost of Innovation and Access
There is also the brutal reality of medical economics. A da Vinci Xi system costs roughly $2 million, plus hundreds of thousands in annual maintenance. These costs are often passed down, or they dictate which hospitals can even offer the "new" procedure. If you live in a rural area, your "new" procedure might still be the laparoscopic method from 2012 simply because of the capital expenditure required for the latest tech. This creates a geographic disparity in outcomes that we don't talk about nearly enough in the glossy brochures of medical tourism. People assume that "standard of care" is a universal constant, but in reality, it is heavily dependent on the zip code of the surgical suite.
Common pitfalls and the mythology of the scalpel
The laser is not a magic wand
The problem is that patients often walk into a consultation demanding a specific brand of laser because they saw a shiny advertisement, yet the hardware matters less than the person holding the fiber. Most men assume that Holmium Laser Enucleation of the Prostate or its Thulium cousin automatically guarantees zero downtime. That is a fantasy. While these "cold" cutting techniques reduce bleeding by approximately 72 percent compared to historical standards, your body still requires a biological grace period to heal the internal raw surface. If you think you are golfing forty-eight hours after a resection, you are setting yourself up for a bloody disappointment. Because the prostate is a highly vascular neighborhood, the new procedure for prostate surgery still involves internal scabbing. Don't let the high-tech marketing fool you into skipping the recovery protocols.
Waiting for total blockage is a disaster
Many guys treat their urinary flow like a dying battery—they wait until it hits zero percent before seeking help. Except that this stoicism backfires. When you delay intervention, the bladder muscle must pump against a stone wall for years, eventually becoming "trabeculated" or permanently thickened and weak. Let's be clear: a perfect surgical result on the prostate cannot fix a bladder that has already surrendered. Data indicates that patients who undergo benign prostatic hyperplasia intervention with a pre-operative bladder capacity below 200ml have a significantly lower satisfaction rate. The surgery clears the pipes, but it cannot jumpstart a dead motor. (Yes, that means your nocturnal bathroom trips might persist if you wait too long.)
The hidden variable: The neurovascular bundle preservation
The millimeter game in the robotic suite
When we discuss the new procedure for prostate surgery, specifically the robotic-assisted radical prostatectomy for oncology cases, the focus usually lands on the robot. The issue remains that the robot is just a high-fidelity puppet. The real "expert secret" lies in the traction applied to the neurovascular bundles during the dissection. Even a microscopic tug can lead to temporary neuropraxia, which explains why some men regain potency in three months while others take two years. Surgeons now utilize a "hydrodissection" technique, using high-pressure saline to gently peel the nerves away from the prostate capsule without heat or physical grasping. This nerve-sparing precision is the difference between biological functionality and lifelong reliance on chemistry. We are moving toward a "total anatomical restoration" where the pelvic floor is reconstructed stitch by stitch to mirror the pre-surgical state. It is tedious work. It is also non-negotiable for quality of life.
Frequently Asked Questions
Will I experience retrograde ejaculation after the procedure?
This remains the most frequent concern for men undergoing transurethral treatments like Aquablation or laser enucleation. Statistics show that traditional TURP resulted in this condition for nearly 65 to 75 percent of patients, but newer "ejaculatory-sparing" protocols have successfully lowered that risk to under 10 percent in specific cohorts. The surgeon must carefully preserve the verumontanum and the surrounding mucosal tissue to maintain the mechanical pathway. As a result: you must prioritize an open dialogue about sexual preservation before the first incision is made. Do not assume the default setting includes these protective maneuvers.
How long does the catheter actually stay in place?
Modern protocols have aggressively slashed the duration of catheterization compared to the five-day marathons of the past. For a standard robotic prostatectomy, most centers now remove the tube within 6 to 8 days, while minimally invasive water-jet treatments often see it gone in 24 to 48 hours. Is it uncomfortable? Absolutely, but it is a temporary necessity to ensure the new urethral connection, or anastomosis, is watertight. Early removal might sound appealing, but premature extraction carries a 4 percent risk of urinary retention, which is a far more painful ordeal than another day with a bag. We balance speed with safety every single time.
Can the prostate tissue grow back after a new procedure?
The prostate is a resilient organ, and while radical surgery removes it entirely, treatments for BPH only remove the obstructive core. Clinical longitudinal studies suggest a re-operation rate of approximately 1 to 2 percent per year following a standard resection. This means after a decade, about 10 to 15 percent of men may require a "touch-up" as the peripheral zone continues its slow, hormonal expansion. Choosing a complete enucleation over a simple vaporization significantly reduces this risk because it reaches the surgical capsule. In short: the more tissue you remove now, the less likely you are to see me again in ten years.
A definitive stance on the future of urology
The era of the "one-size-fits-all" prostatectomy is dead, and frankly, it deserved to die. We have entered a phase of hyper-personalization where the choice of a new procedure for prostate surgery depends entirely on the cubic centimeter volume of your gland and your personal tolerance for side effects. It is no longer enough to just "be able to pee" or "be cancer-free" as the bare minimum. We must demand functional excellence, which includes urinary continence and sexual health as primary metrics of success. The technology is finally caught up to our ambitions, but only if the patient remains an active, informed pilot rather than a passive passenger. My position is simple: if your surgeon cannot explain the specific nerve-sparing technique they use, find a different surgeon. Precision is the only currency that matters in the pelvis. We are not just removing a blockage; we are salvaging a lifestyle.