The Fluid Mechanics of Human Circulation: Moving Past the Baseline Numbers
Why Your Arteries Aren't PVC Pipes
Blood pressure isn't a static number. Your heart pumps roughly five liters of blood per minute through an incredibly intricate, living web of vessels that dilate and constrict based on stress, posture, and metabolic demand. When the left ventricle contracts—a phase known as systole—it hurls blood against the arterial walls with tremendous force. This creates the top number, the systolic pressure. The bottom number, or diastolic pressure, measures the residual force when the heart rests between beats. The thing is, mainstream medicine treats these two metrics as immutable laws cast in stone, ignoring the basic biological reality that human tissues degrade, change composition, and lose elasticity over time. It is a dynamic system, not plumbing.
The Statistical Tyranny of the 120/80 mmHg Target
Where it gets tricky is the historical origin of these metrics. For decades, global health bodies like the American Heart Association and the European Society of Cardiology pooled vast epidemiological data to establish a clean, memorable threshold. Normal blood pressure became defined globally as less than 120/80 mmHg. But people don't think about this enough: these guidelines are heavily driven by large-scale pharmaceutical trials designed for population-wide risk reduction rather than individualized clinical nuance. I believe this obsession with a single idealized metric has caused millions of older adults to be aggressively over-medicated. We see patients dizzy, falling, and suffering from orthostatic hypotension just so a computer chart can show a pristine, youthful reading. It is absurd.
The True Trajectory: How Perfect Blood Pressure by Age Shifts Across Decades
The Youthful Baseline: Age 18 to 39
During early adulthood, the vascular system possesses maximum compliance. The collagen matrices within the aortic wall are intact, and elastin fibers bounce back effortlessly after every single cardiac contraction. For a twenty-five-year-old woman in Boston or a thirty-year-old man in London, a reading of 115/75 mmHg is arguably the true biological ideal. Because young vessels absorb the kinetic energy of the pulse wave so effectively, the systolic pressure naturally stays low. If a thirty-year-old consistently registers 135/85 mmHg, it signals premature vascular aging, likely driven by metabolic dysfunction, chronic sleep deprivation, or systemic inflammation. Here, the strict guidelines make sense.
The Midlife Pivot: Age 40 to 59
Then comes the middle-age shift. Somewhere around the mid-forties, the micro-vessels feeding the arterial walls—the vasa vasorum—begin to show subtle signs of degradation, which explains why the systolic number naturally begins its upward creep. For individuals in this bracket, achieving what is perfect blood pressure by age means recognizing that a systolic reading of 120 to 128 mmHg is not a crisis, even if it technically gets flagged as prehypertension. Yet, doctors frequently reach for the prescription pad at the first sight of a 132/82 mmHg reading in a fifty-year-old corporate executive. This overlooks the fact that the body is simply compensating for a natural, unavoidable decrease in vessel compliance. Is a minor elevation really a pathology, or is it just the body maintaining adequate organ perfusion? The issue remains highly debated among progressive cardiologists who favor lifestyle interventions over immediate chemical intervention at this stage.
The Geriatric Paradox: Age 60 and Beyond
This is where conventional wisdom completely unravels. Once a person crosses the threshold of sixty-five, the large arteries undergo a process called medial calcification. They stiffen. As a result, the systolic pressure jumps while the diastolic pressure frequently drops, a phenomenon known as isolated systolic hypertension. In an eighty-year-old patient, a blood pressure of 135/70 mmHg or even 140/75 mmHg may actually be optimal for preserving cognitive function and renal perfusion. If you force that person's systolic pressure down to 115 mmHg using a cocktail of beta-blockers and diuretics, you risk starving the brain of oxygenated blood. We are far from the simple mechanics of youth here. Honestly, it's unclear why the medical establishment remains so resistant to adopting formalized, age-stratified targets, except that uniform guidelines are far easier to teach and market.
The Critical Data Points: What the Landmark Clinical Trials Actually Revealed
Deconstructing the SPRINT Trial and Its Fallout
To understand the current obsession with aggressive lowering, we must examine the Systolic Blood Pressure Intervention Trial (SPRINT) published in late 2015. This massive study randomized over nine thousand participants aged fifty and older to either a standard systolic target of 140 mmHg or an intensive target of 120 mmHg. The researchers concluded that the intensive group experienced significantly lower rates of cardiovascular events. Except that the method used to measure blood pressure in SPRINT was highly unusual—investigators used automated, unobserved office blood pressure measurements, where the patient sat alone in a quiet room for several minutes before the machine activated automatically. This specific technique yields readings that are routinely 5 to 10 mmHg lower than standard clinical measurements! When busy doctors applied the SPRINT targets to real-world patients using traditional cuff techniques, they inadvertently pushed real-world systolic numbers down to dangerously low levels, causing widespread episodes of acute kidney injury and fainting.
The J-Curve Phenomenon in Elderly Populations
The danger of over-treating blood pressure in older demographics is perfectly illustrated by the J-curve concept. This physiological principle demonstrates that while mortality risk drops as blood pressure decreases, it hits a floor and then dramatically spikes upward if the pressure falls too low. A landmark 2018 study analyzing health records of over twenty thousand elderly patients in the United Kingdom confirmed that those with a systolic pressure lowered below 120 mmHg had a significantly higher mortality rate than those maintained between 130 and 139 mmHg. The heart is a pump that requires a certain amount of backpressure to fill the coronary arteries during diastole. If you strip that pressure away, the myocardium itself suffers from subclinical ischemia.
The Disconnect: Standard Guidelines vs. Real-World Longevity Targets
A Comparative Breakdown of Ideals Across the Lifespan
To cut through the confusion, we need a clear comparison between what the strict guidelines demand and what clinical longevity specialists actually target in practice. The discrepancy highlights the gulf between population-level management and individualized care. Consider this breakdown of realistic, age-adjusted optimal ranges for healthy individuals without severe comorbidities like advanced diabetes or end-stage renal disease.
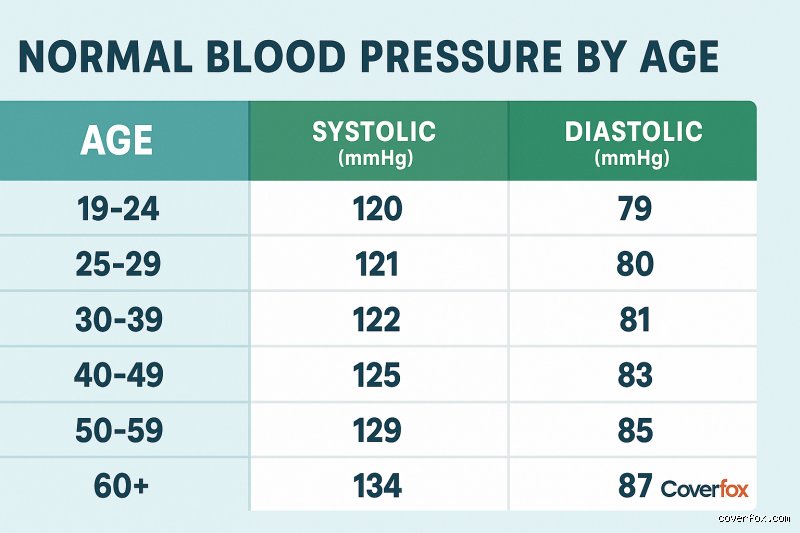
For young adults aged 18 to 39, the traditional guideline is less than 120/80 mmHg, and the longevity target matches closely at 110-118/70-78 mmHg. For middle-aged adults aged 40 to 59, standard metrics still demand less than 120/80 mmHg, but a pragmatic longevity target allows for 120-128/75-82 mmHg to ensure adequate coronary flow without inducing chronic vascular stress. For older adults aged 60 to 74, guidelines reluctantly tolerate up to 130/80 mmHg, whereas real-world longevity experts look for 125-135/75-80 mmHg. Finally, for the elderly population aged 75 and above, where the guidelines still push for aggressive reduction, a safe, rational longevity target is 130-142/70-80 mmHg to prevent cerebral hypoperfusion and debilitating falls. Hence, looking at a single chart on a clinic wall is completely insufficient for determining your actual cardiovascular risk profile.
The Hidden Threat of Widening Pulse Pressure
Another crucial metric that people don't think about enough is pulse pressure, which is simply the mathematical difference between your systolic and diastolic numbers. If your reading is 140/80 mmHg, your pulse pressure is 60 mmHg. A widening pulse pressure—anything above 50 mmHg—is an incredibly strong independent predictor of heart attacks and strokes in older individuals because it serves as a direct proxy for arterial stiffness. A patient with a reading of 138/70 mmHg might have a seemingly acceptable systolic number, but that sixty-eight-point gap tells a story of rigid, calcified vessels that can no longer cushion the heart's output. In these scenarios, focusing solely on driving down the systolic number can cause the diastolic number to plummet even further, worsening the overall clinical picture. The entire hemodynamical landscape must be evaluated together.
Common mistakes and dangerous misconceptionsThe "My natural number" trap
You probably think your baseline is just yours to keep. The problem is that a reading of 140/90 mmHg at age sixty-five is not a benign badge of seniority. Many seniors assume aging grants a biological pass for stiffer plumbing. It does not. Systolic creep delivers stroke risks regardless of your birth certificate, meaning that normalized high readings remain lethal. Let's be clear: letting your numbers drift upward just because your peers have done so is a massive gamble. But your arteries do not grade on a curve.
The white-coat overcorrection
White-coat hypertension is notoriously real, yet the inverse reaction can be equally disastrous. Patients routinely dismiss a high reading in the clinic by blaming the traffic, the parking meter, or the cold stethoscope. Which explains why true, masked hypertension goes completely undetected for years until organ damage occurs. You cannot simply delete an unfavorable metric because you felt anxious. It is a data point, not an insult. Instead, consistent home monitoring with an validated arm cuff remains the definitive method to unmask your genuine cardiovascular baseline.
Ignoring the lower number in youth
Younger adults under forty frequently obsess over the top number while ignoring isolated diastolic hypertension. A bottom reading consistently hovering at 95 mmHg indicates high systemic vascular resistance. Except that young people feel invincible, so they skip the screening entirely. Diastolic spikes damage delicate kidney capillaries long before the classic cardiac symptoms manifest. And ignoring this early warning sign essentially guarantees structural vascular remodeling by middle age.
The hidden variable: Arterial stiffness and pulse pressure
Why the gap between numbers matters most
Everyone looks at the absolute values, but the real diagnostic gold lies in the math between them. Pulse pressure is the specific mathematical difference between your systolic and diastolic measurements. As we age, large elastic arteries lose their compliance, a phenomenon that causes the top number to skyrocket while the bottom number drops. A reading of 160/60 mmHg gives a pulse pressure of 100 mmHg, which signals highly rigid, compromised vessels. What is perfect blood pressure by age if your pulse pressure indicates your aorta has turned to stone? The issue remains that clinicians often treat the high systolic while inadvertently driving the diastolic dangerously low, compromising coronary perfusion. Striking the balance requires looking at the hemodynamic trend, not just isolated targets. (This is why geriatric cardiology requires a delicate touch rather than aggressive, blanket medication protocols).
Frequently Asked Questions
Does what is perfect blood pressure by age change if you have diabetes?
Yes, the presence of metabolic disease completely rewrites the cardiovascular rulebook. For an average healthy fifty-year-old, a reading of 125/80 mmHg is perfectly acceptable, but a diabetic patient requires a stricter threshold of less than 130/80 mmHg according to standard clinical guidelines. High blood glucose levels synergyistically accelerate arterial damage, which doubles the risk of diabetic nephropathy and retinopathy. As a result: keeping pressure lower mitigates the cumulative microvascular destruction. Consequently, therapeutic intervention begins much earlier for diabetic individuals to preserve renal function.
How does physical fitness alter the expected blood pressure norms?
Endurance athletes frequently exhibit resting readings that look shockingly low to the untrained eye, often averaging around 100/60 mmHg. This occurs because chronic aerobic training expands stroke volume and enhances vagal tone, allowing the heart to pump more blood with fewer contractions. The resting vascular bed remains highly dilated and compliant. In short, your fitness level shifts your personal ideal well below the standard population averages without causing any symptoms of hypotension. However, these low numbers are a sign of elite efficiency rather than pathology, provided there is no accompanying dizziness.
Can short-term stress permanently alter my age-based baseline?
Acute stress spikes cortisol and adrenaline, causing transient surges that do not reflect your true arterial health. However, chronic allostatic load from years of high-stress employment can permanently alter your neurohormonal baseline. The sympathetic nervous system becomes chronically overactive, preventing the blood vessels from returning to a relaxed state. Therefore, while a single stressful meeting won't permanently change your ideal metrics, a decade of constant pressure will fundamentally alter your resting physiology.
A definitive stance on vascular aging
We must stop treating what is perfect blood pressure by age as a sliding scale that forgives physical decline. Allowing target numbers to loosen as the population ages is a philosophy driven by complacency rather than optimal physiology. The human heart requires a stable pressure gradient to thrive, and letting the ideal threshold rise over time merely normalizes systemic arterial decay. While aggressive medication in fragile octogenarians carries distinct risks, our primary preventive goal should always aim for youthful vascular elasticity. Compromising on target numbers because a patient has crossed an arbitrary age threshold is an outdated approach. We should fight to maintain low pressure from youth through old age, using lifestyle as our primary weapon. Your blood vessels do not care about your chronological age; they only respond to the constant, hydraulic force tearing at their walls every single day.