The Anatomy of Deception: Why We Call It a False Aneurysm
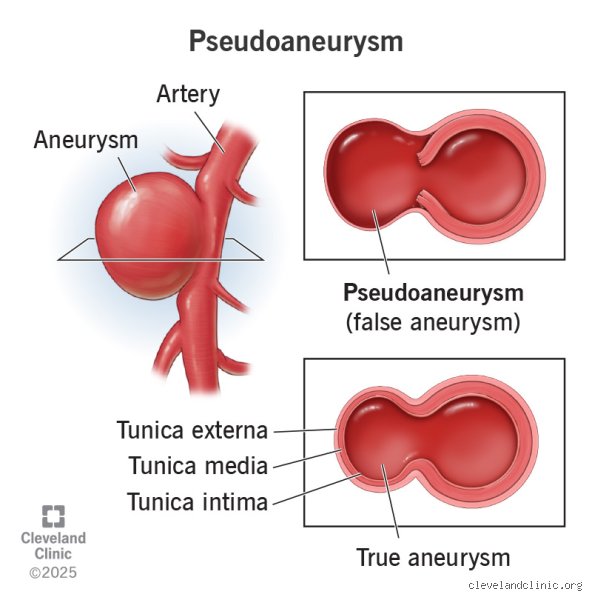
To get our heads around this, we first need to scrap the idea that all bulges in the blood vessels are created equal. A true aneurysm involves the stretching of all three layers of the arterial wall—the intima, media, and adventitia—much like a balloon that has been inflated too many times. But a pseudoaneurysm? That is a different beast entirely. It is essentially a contained hematoma that maintains a persistent, violent communication with the high-pressure arterial lumen. Because the structural integrity of the artery is gone, the "wall" of this new sac is nothing more than compressed soft tissue or a thin shell of thrombus. Honestly, it is a structural miracle that these things don't burst immediately upon formation, yet they can sit there for days or weeks, pulsing away under your skin like a hidden heartbeat.
When the Pressure Cooker Meets the Skin
But here is where it gets tricky for the average person to spot the difference. In a standard "bleed," you might see a bruise (ecchymosis) or feel a soft swelling that eventually stabilizes as the body’s clotting factors do their heavy lifting. In the case of a pseudoaneurysm, the blood is still very much a part of the party, rushing in and out of the sac with every single contraction of the heart. This creates a palpable thrill or a "bruit" that a doctor can hear through a stethoscope—a rhythmic whooshing sound that signals the blood is trapped in a swirling, turbulent vortex. I find it fascinating that such a violent internal event can sometimes look like nothing more than a slightly painful lump to the untrained eye.
The Mechanics of Rupture and the Myth of Stability
People don't think about this enough: a pseudoaneurysm is effectively a failure of the healing process. When an interventional cardiologist pulls a sheath out of a femoral artery after a stent placement, or when a piece of shrapnel nicks a vessel in a freak accident, the hole is supposed to seal. If it doesn't, and the blood finds a pocket in the nearby fascia to call home, you have extravasation without evacuation. Experts disagree on exactly how long a pseudoaneurysm can remain "stable" before it decides to ruin someone's Tuesday. Some small ones, perhaps under 2 centimeters in diameter, might actually clot off and disappear on their own through spontaneous thrombosis. Yet, for larger ones, the sheer hemodynamic stress usually wins out, leading to a catastrophic rupture that turns a contained problem into a massive, life-threatening hemorrhage in seconds.
The Femoral Artery: A Case Study in Medical Risk
Take, for example, the common femoral artery, which is the most frequent site for these complications following cardiac catheterization procedures. Data from large-scale clinical registries suggests that the incidence of pseudoaneurysm can range from 0.2% to as high as 8% depending on the complexity of the intervention and whether the patient is on aggressive anticoagulants like heparin or warfarin. If you are a 70-year-old patient who just had a TAVR (Transcatheter Aortic Valve Replacement) in Chicago, and you notice a hard, painful lump in your groin three days later, that isn't just a bruise. That is the arterial pressure trying to find a new, weaker path. The issue remains that the skin and muscle are never meant to hold back the 120 mmHg of pressure your heart generates, which explains why these "false" aneurysms are so prone to sudden failure.
The Role of Turbulent Flow and the Ying-Yang Sign
When a radiologist looks at a suspected pseudoaneurysm through a Color Doppler Ultrasound, they aren't just looking for a pocket of fluid. They are looking for the "Ying-Yang sign." This distinctive visual pattern shows blood swirling into the sac (red) and then back out into the artery (blue) in a constant, chaotic loop. It is a beautiful image for a textbook but a nightmare for the patient's physiology. Because the blood is moving so fast and with such force, it prevents a solid clot from forming at the neck of the leak. As a result: the pocket grows. It isn't just "bleeding" in the sense of losing volume; it is displacing anatomy, pushing on nerves, and potentially cutting off circulation to the rest of the limb.
Distinguishing the Clinical Presentation: Bleeding vs. Pseudoaneurysm
Is it possible to tell them apart without a million-dollar imaging suite? Sometimes, but we're far from it being a simple DIY diagnosis. Traditional internal bleeding often presents with a drop in blood pressure, a rising heart rate, and a general sense of impending doom as the hemoglobin levels plummet. A pseudoaneurysm, conversely, might not affect your systemic blood pressure at all, at least not initially. The blood is "lost" from the vessel but still "stored" locally. This can lead to a false sense of security. You might feel fine, except for a localized ache, while a 500ml hematoma is slowly expanding under your thigh muscle, compressing the femoral nerve and risking permanent paralysis of the quadriceps.
The Danger of the "Silent" Expansion
And that changes everything when it comes to the urgency of treatment. If a nurse sees an active bleed, they apply manual pressure immediately—sometimes for 30 or 40 minutes—to force the body to clot. But if that pressure is applied incorrectly to a pseudoaneurysm, or if the "neck" of the leak is too wide, the pressure does nothing but cause immense pain. In fact, if the sac is close to the skin, it can cause skin necrosis. The pressure from within cuts off the blood supply to the skin itself, causing the tissue to die and turn black. I've seen cases where a neglected pseudoaneurysm eventually eroded right through the surgical scar, leading to a "blowout" that no amount of gauze could stop. We have to stop viewing these as static lumps and start seeing them as dynamic, evolving lesions.
Alternative Realities: Hematomas, Seromas, and Other Mimics
Of course, not every bump after a needle poke is a pseudoaneurysm, which is why the diagnostic process is such a minefield. A simple hematoma is just a collection of clotted blood—it doesn't "talk" back to the artery. Then you have seromas, which are collections of sterile fluid that can appear after surgery. The issue remains that these are passive, while the pseudoaneurysm is active. In some rare instances, patients might even develop an arteriovenous fistula, where the needle has accidentally created a tunnel between an artery and a vein. This also creates a bruit and a thrill, but instead of a sac, the blood is short-circuiting the entire capillary system. Hence, the "bleeding" is happening internally, but it’s going into the venous system instead of a tissue pocket. Every one of these requires a different surgical or radiological approach, making the "is it bleeding?" question almost too simple for the reality of the situation.
Why the "Watch and Wait" Approach is Controversial
Historically, surgeons were quick to cut. If they saw a pseudoaneurysm, they opened the patient up and stitched the artery shut. Today, we have moved toward ultrasound-guided thrombin injection, where a doctor literally injects a clotting agent directly into the sac to turn it into a solid, harmless brick of protein. But some experts still argue for observation in small, asymptomatic cases. Is it worth the risk? If the patient is on dual antiplatelet therapy (DAPT) after a heart attack, the chances of that hole closing on its own are slim to none. In my view, the nuance of the patient's overall health profile is often ignored in favor of strict "size-based" guidelines, which is a mistake because a small leak in an old, friable artery is far more dangerous than a larger one in a healthy 20-year-old athlete.
Common pitfalls and the trap of the visual
People often conflate "bleeding" with the dramatic imagery of a ruptured pipe, yet a pseudoaneurysm behaves with a far more insidious logic. The problem is that many clinicians and patients assume that if there is no external hemorrhage or rapidly expanding hematoma, the vessel is secure. This is a fallacy. Let's be clear: a false aneurysm is a leak that has simply run out of room for the moment. Because the blood is contained by a thin, fibrous wall of adventitia or surrounding soft tissue rather than the trivalent arterial structure, it is a ticking clock. It is not "stable" bleeding; it is a pressurized mistake waiting for a reason to fail.
The diagnostic mirage of the bruise
Is a pseudoaneurysm the same as bleeding when you only see a purple patch on the skin? Hardlly. A common mistake is dismissing a post-procedural site as a simple bruise or a standard hematoma. While a hematoma is a clotted collection of stagnant blood, a pseudoaneurysm maintains a functional connection to the arterial lumen. This means blood is actively swirling in and out of the sac through a narrow neck. In about 2% to 3% of femoral artery access cases, this distinction is missed because the observer lacks the tactile sensitivity to feel for a "thrill" or a palpable pulsation. If you ignore the pulse, you ignore the pathology.
Misinterpreting the ultrasound silence
Relying solely on B-mode ultrasound without color Doppler is a recipe for disaster. Why would anyone skip the color flow? Without it, the sac may appear as a static fluid collection, mimicking an abscess or a cyst. The "yin-yang" flow pattern—the swirling red and blue of blood entering and exiting—is the pathognomonic hallmark that separates a pseudoaneurysm from a simple internal bleed. As a result: failure to utilize hemodynamic imaging leads to inappropriate needle aspirations, which can cause catastrophic, uncontainable hemorrhage when a needle punctures a high-pressure arterial leak disguised as a fluid pocket.
The hemodynamic ghost: A little-known expert perspective
Medical professionals often focus on the anatomy, but we need to talk about the bio-mechanical fatigue of the surrounding tissue. When blood escapes the artery but stays trapped, it creates a localized inflammatory response. This inflammation effectively "digests" the nearby fascia. But here is the kicker: the very wall holding the blood in is often composed of the same inflammatory debris it is trying to contain. It is an architectural nightmare. We have seen cases where the pseudoaneurysm wall is so friable that it cannot hold a suture, turning a relatively minor repair into a complex vascular reconstruction. The issue remains that we treat the hole, but we often forget to respect the compromised integrity of the landing zone around it.
The thrombin injection nuance
There is a prevailing myth that every pseudoaneurysm requires a scalpel. This is outdated thinking. For many, ultrasound-guided thrombin injection is the gold standard, boasting success rates over 90%. Yet, the expert's secret lies in the neck of the sac. If the neck is too wide, the thrombin can escape into the main arterial flow, causing distal embolization and potential limb loss. You must possess the technical grit to hold the transducer perfectly still while the chemical reaction occurs. (This is significantly harder than it sounds when a patient is moving). In short, the "bleeding" is controlled by turning the blood into a solid plug, but the margin for error is razor-thin.
Frequently Asked Questions
Can a pseudoaneurysm heal on its own without intervention?
Small lesions under 2 centimeters in diameter occasionally undergo spontaneous thrombosis, particularly if the patient is not on aggressive anticoagulation therapy. Data suggests that roughly 30% to 50% of these tiny defects might close within four weeks of observation. However, this is a gamble that requires frequent surveillance via duplex ultrasound to ensure the sac is not expanding. The risk of rupture remains a constant shadow during this "wait and see" period. But relying on luck is rarely a sound clinical strategy when dealing with high-pressure arterial systems.
How long after a surgery can a pseudoaneurysm appear?
While most present within the first 24 to 48 hours post-trauma or catheterization, delayed presentations can occur weeks later. In orthopedic cases involving hardware, a delayed pseudoaneurysm might manifest 3 to 6 months after the initial surgery due to chronic friction between a screw and an artery. Statistics indicate that late-onset cases account for less than 5% of total diagnoses, but they often carry higher morbidity because the initial surgical trauma is long forgotten. You must remain vigilant for any new pulsatile swelling, even months after the "all-clear" was given.
What is the mortality rate if a pseudoaneurysm actually ruptures?
The mortality rate for a ruptured pseudoaneurysm varies wildly depending on the location, with visceral artery ruptures carrying a staggering 25% to 70% death rate. If an extracranial carotid pseudoaneurysm fails, the risk of stroke or lethal exsanguination is nearly immediate. In contrast, femoral ruptures are easier to compress but still lead to significant blood loss and limb ischemia if not addressed in minutes. The issue remains that "bleeding" into a cavity like the abdomen is silent until the patient's blood pressure bottoms out. Which explains why we treat these as surgical or interventional emergencies rather than elective inconveniences.
A definitive stance on the vascular paradox
Calling a pseudoaneurysm "bleeding" is like calling a live grenade "fire"—it ignores the structural tension that makes the situation explosive. We must stop using these terms interchangeably in clinical settings to prevent a dangerous dilution of urgency. A pseudoaneurysm is a hemodynamic failure of the vessel wall that demands a unique, targeted response. It is the most deceptive form of vascular injury because it masquerades as a stable collection while harboring the full pressure of the heart. Except that we have the tools to stop it, provided we stop underestimating the physics of the leak. My position is firm: every pseudoaneurysm is an active threat until proven thrombosed. The difference between a controlled sac and a lethal hemorrhage is often just a few millimeters of bruised tissue and a heavy dose of misplaced optimism.