The Hidden Chemical Factory: Understanding Pancreatitis and Why Tissue Integrity Matters
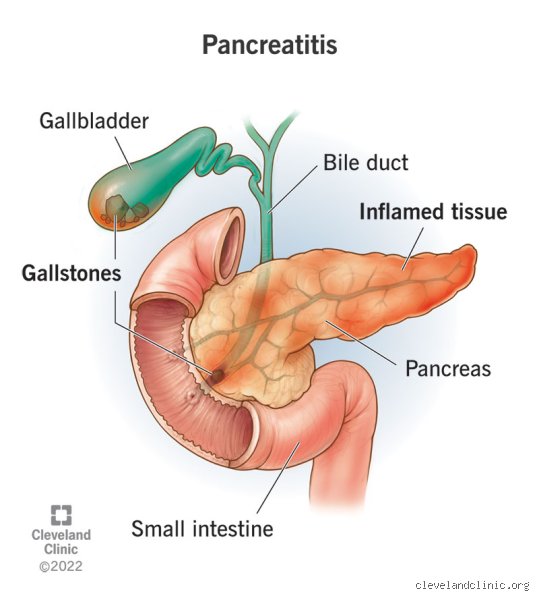
To understand if the organ can mend, we first need to look at what happens when the system goes rogue. Your pancreas is a dual-purpose powerhouse, operating both as an exocrine gland producing digestive enzymes like trypsin, protease, and lipase, and as an endocrine gland pumping insulin directly into your bloodstream. Pancreatitis occurs when these digestive juices, which are normally safely deactivated until they reach the duodenum, suddenly trigger prematurely inside the pancreas itself. It is a literal process of self-digestion.
Acute Versus Chronic States: The Divergent Paths of Cellular Survival
The difference between the two forms of this condition is night and day. Acute pancreatitis is a sudden, violent storm. It often hits out of nowhere—frequently triggered by a stray gallstone blocking the pancreatic duct at the Ampulla of Vater or a sudden binge of heavy alcohol consumption. But here is where it gets tricky: despite the agonizing pain that sends over 275,000 Americans to the emergency room annually, the tissue structure usually remains intact once the initial fire is put out. Chronic pancreatitis, on the other hand, is a slow, smoldering burn that quietly hollows out the organ over a decade.
The Anatomy of Destruction: Acinar Cells on the Brink
When the internal plumbing fails, the specialized acinar cells bear the brunt of the trauma. In a healthy state, these cells are masterpieces of cellular transport, packaging dangerous enzymes into zymogen granules. During an attack, these granules rupture internally. The resulting cellular necrosis triggers a massive influx of inflammatory cytokines, which explains why patients experience such profound, radiating back pain. If the basement membrane of the tissue remains undamaged during this onslaught, the organ retains its architectural blueprint, allowing a complete structural rebuild.
The Biological Blueprint of Healing: How the Pancreas Initiates Self-Repair
Can your pancreas heal itself from pancreatitis? At a microscopic level, the body possesses an astonishing, albeit fragile, toolkit for renewal. Once the offending trigger—whether that is a gallstone, a medication like azathioprine, or high blood triglycerides—is removed, the organ immediately shifts from a state of hyper-inflammation to a highly coordinated phase of cellular proliferation.
The Unsung Heroes: Pancreatic Stellate Cells and the Fibrosis Trap
We need to talk about pancreatic stellate cells because people don't think about this enough. In a quiescent state, these cells merely store vitamin A and mind their own business. Yet, the moment acute injury strikes, they transform into myofibroblast-like entities. They rush to the scene of the injury to lay down a temporary extracellular matrix, acting as a biological scaffold. But this is a double-edged sword; if the inflammation does not subside quickly, these cells keep churning out collagen type I and III, leading to irreversible fibrosis. This is the exact tipping point where self-repair fails and permanent scarring wins.
Regeneration Mechanics: Acinar-to-Ductal Metaplasia
How do new cells actually form when half the tissue has been obliterated by auto-digestion? The answer lies in a fascinating shape-shifting process called acinar-to-ductal metaplasia, or ADM. Surviving acinar cells temporarily dedifferentiate into a primitive, duct-like state, mimicking embryonic development. These transient cells rapidly multiply to replenish the lost biomass, before transitioning back into mature, functioning acinar units. It is an elegant survival mechanism, except that if oncogenic mutations like KRAS are present, this exact regenerative pathway can accidentally veer off-course into pancreatic ductal adenocarcinoma.
The Structural Point of No Return: When Self-Healing Becomes An Impossible Dream
I must take a firm stance here against the alternative wellness narratives claiming that a specific juice cleanse or herbal protocol can reverse long-term pancreatic damage. They cannot. Once the organ crosses a specific threshold of structural degeneration, the innate capacity for self-repair vanishes completely, leaving behind a non-functioning, fibrotic shell.
The Tipping Point: Defining the Ammann Criteria for Chronic Disease
Medical historians and gastroenterologists often point to the Ammann criteria, developed through decades of clinical observation in Zurich, which outlines the progression of alcoholic chronic pancreatitis. The disease follows a predictable, devastating trajectory. After repeated acute flares, the continuous activation of stellate cells plugs the pancreatic ducts with protein precipitates. These plugs eventually calcify into stones, entirely choking off the flow of digestive enzymes. At this stage, the functional parenchyma is permanently replaced by dense, useless connective tissue.
Endocrine Bankruptcy: The Onset of Type 3c Diabetes
What happens when the destruction spreads from the exocrine tissue to the endocrine microenvironment? The Islets of Langerhans, which house the precious beta cells responsible for producing insulin, are typically resilient, but they are not invincible. Continuous, unremitting inflammation eventually decimates these islet clusters. The result is pancreatogenic diabetes, scientifically classified as Type 3c diabetes. Unlike standard Type 2 diabetes, which is characterized by insulin resistance, Type 3c is a state of absolute insulin deficiency combined with a total loss of glucagon production from alpha cells, making blood sugar management an absolute nightmare for clinicians.
Quantifying Recovery: Comparing Acute Resolution Against Chronic Management
The timeline and success rate of pancreatic healing vary wildly depending on the severity of the initial insult and the baseline health of the patient. Let us look at the hard data to understand what recovery actually looks like in a clinical setting.
Mild Acute Pancreatitis: The Best-Case Scenario
For patients diagnosed with interstitial edematous pancreatitis—which accounts for roughly 80% of all acute admissions—the prognosis is remarkably reassuring. In these cases, inflammation is confined to tissue swelling without any cellular death. Within 3 to 5 days of bowel rest, aggressive intravenous fluid resuscitation with lactated Ringer's solution, and targeted pain management, the pancreas clears the inflammatory debris. Studies show that within 4 to 6 weeks, full exocrine and endocrine function is typically restored, leaving no permanent deficit behind.
Severe Necrotizing Pancreatitis: The Critical Midpoint
Where it gets truly dangerous is when the acute attack progresses to necrotizing pancreatitis, a condition where portions of the tissue lose their blood supply and die. This affects about 20% of patients and carries a mortality rate that can exceed 30% if the dead tissue becomes infected with bacteria migrating from the colon. Healing here is a grueling, multi-month marathon often requiring minimally invasive debridement procedures like the retroperitoneal approach. While the surviving segments of the pancreas will attempt to hypertrophy to compensate for the lost tissue, patients are frequently left with a permanent reduction in digestive capacity, requiring lifelong pancreatic enzyme replacement therapy to avoid malabsorption and steatorrhea.
Common myths blocking pancreatic recovery
The "just a liquid diet" illusion
People assume that sipping broth for forty-eight hours magically resets a deeply inflamed organ. It does not. While resting the digestive tract prevents the organ from pumping out destructive enzymes prematurely, self-prescribed starvation often backfires spectacularly. The problem is that malnutrition actively cripples cellular repair. Your acinar cells require a massive influx of amino acids to rebuild their shattered architecture after an acute flare-up. Skipping solid food without medical supervision deprives the body of the exact raw materials needed for tissue regeneration. Malnutrition delays pancreatic healing by stalling the cellular synthesis required to replace dead tissue, turning a temporary insult into a prolonged crisis.
The trap of the "occasional" drink
Let's be clear: there is no safe margin for alcohol consumption once this gland has been compromised. Patients frequently believe that transitioning from heavy drinking to a single glass of red wine during social gatherings is harmless. Except that your acinar cells develop an extreme, long-lasting hypersensitivity to ethanol metabolites after an initial inflammatory event. Even a microscopic dose of alcohol can trigger premature zymogen activation inside the tissue, causing the organ to literally digest itself all over again. Alcoholic pancreatitis requires absolute abstinence to prevent irreversible fibrotic scarring. Why risk permanent organ failure for a fleeting social lubricant?
Misjudging over-the-counter enzymes
Pop a pill, eat a steak, right? Wrong. Buying random pancreatic enzyme replacement therapies online without a specific prescription usually amounts to expensive placebo usage. Unregulated supplements frequently degrade in stomach acid before they ever reach the duodenum. Exocrine pancreatic insufficiency demands pharmaceutical-grade enzymes that are precisely enteric-coated to survive gastric pH levels. Taking under-dosed over-the-counter alternatives creates a false sense of security while your body continues to suffer from severe malabsorption and progressive nutritional deficiencies.
The hidden microvascular battlefield of pancreatic repair
Angiogenesis determines structural survival
We rarely talk about blood vessels when discussing how this organ mends, yet the microcirculation network holds the real key to long-term recovery. During severe acute attacks, the localized inflammatory cascade causes widespread endothelial dysfunction and microscopic blood clots. Ischemia-induced necrosis prevents tissue regeneration because oxygen and vital nutrients simply cannot reach the damaged areas. If the capillary network does not rebuild itself through angiogenesis, the dead patches of the gland will inevitably transform into rigid, non-functional scar tissue instead of healthy parenchymal cells. Can your pancreas heal itself from pancreatitis if its blood supply is completely choked off? Absolutely not.
This is where targeted medical intervention becomes fascinating. Advanced clinical protocols now focus heavily on protecting the pancreatic microvasculature during the early stages of hospitalization. Aggressive, carefully calculated intravenous hydration therapy is used to maintain capillary perfusion pressures. (We must admit that balancing fluid resuscitation without causing pulmonary edema remains an incredibly delicate tightrope walk for ICU physicians). Early microvascular protection reduces permanent scarring, which explains why identical initial attacks can lead to completely different long-term health outcomes for different patients depending on how quickly aggressive fluid therapy was initiated.
Frequently Asked Questions
How long does it take for pancreatic inflammation to fully subside?
Mild cases of acute inflammation typically resolve within three to seven days of standard supportive hospital care. However, the underlying cellular recovery process continues silently beneath the surface for several weeks after your symptoms disappear. Complete structural stabilization takes up to six months according to longitudinal imaging studies tracking tissue density. Data indicates that approximately twenty percent of patients experiencing a severe acute episode develop localized fluid collections or pseudocysts that require up to twelve weeks to spontaneously reabsorb. If necrosis has occurred, the timeline extends indefinitely as the organ permanently remodels its architecture around the damaged zones.
Can a lifestyle change reverse chronic pancreatic scarring?
Once fibrotic tissue replaces healthy parenchymal cells, that specific structural damage becomes permanent and irreversible. You cannot scrub away the physical scars left behind by chronic inflammation. But a strict, permanent shift in daily habits halts the progressive destruction of the remaining functional tissue. A low-fat diet under thirty grams daily drastically reduces the metabolic workload placed on the organ, preventing further inflammatory flare-ups. Clinical registries show that patients who achieve total smoking cessation reduce their risk of disease progression by nearly forty percent compared to those who continue lighting up.
What are the definitive signs that the organ is not recovering properly?
Persistent, gnawing pain that radiates directly into your upper back indicates that chronic inflammation is actively setting in. Another alarming red flag is the sudden appearance of oily, foul-smelling stools that float in the toilet bowl, a condition known medically as steatorrhea. Steatorrhea signifies over ninety percent exocrine destruction, meaning the organ can no longer produce adequate amounts of lipase to break down dietary fats. Unexplained, rapid weight loss despite consuming normal amounts of food also proves that nutrient malabsorption has reached a critical threshold requiring immediate medical intervention.
A definitive medical stance on pancreatic recovery
Passive waiting is a recipe for permanent metabolic disaster. The human body possesses remarkable regenerative capabilities, but this particular organ operates on a knife-edge where unmanaged inflammation rapidly accelerates into irreversible fibrosis. You cannot simply wish your way back to health without radically altering your relationship with nutrition and toxins. Proactive lifestyle modification dictates your long-term prognosis far more than any temporary medical intervention. Relying on luck or half-measures will eventually result in brittle diabetes and chronic malabsorption. Take absolute control of your recovery protocol immediately because your digestive survival depends entirely on the choices you make today.