The Messy Reality of Defining a Neurodegenerative Timeline
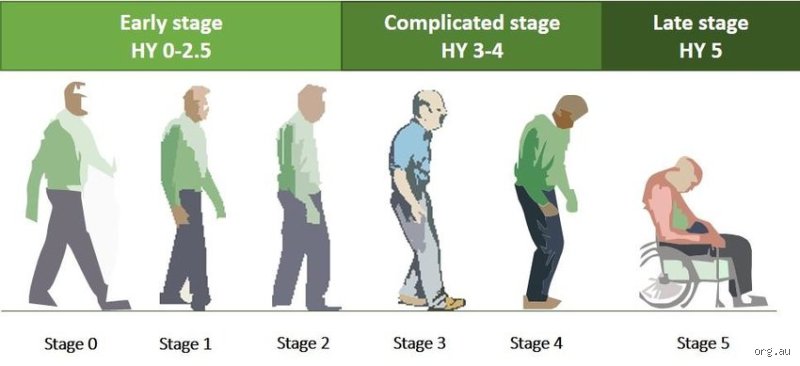
We love to neatly categorize medical conditions because chaos scares us. When Margaret Hoehn and Melvin Yahr published their groundbreaking rating system in the journal Neurology back in 1967, they gave the medical community a brilliant, much-needed map. Yet, modern neurology often clings to these five phases too rigidly. Parkinson’s is not a staircase where you finish step one and neatly land on step two. People don't think about this enough, but a patient can experience the cognitive shifts of an advanced stage while their physical mobility remains anchored in the earliest phase. It is an erratic, highly individualized breakdown of the substantia nigra.
Why the Hoehn and Yahr Scale Both Helps and Fails Us
The scale focuses almost exclusively on objective motor signs. It measures things doctors can see in a clinic exam room, like postural instability, rigid limbs, and that classic, rhythmic pill-rolling resting tremor. Except that it completely ignores the invisible, non-motor symptoms that often break a person's spirit long before their balance goes out the window. Severe depression, REM sleep behavior disorder, and a phantom-like loss of smell frequently predate any physical shaking by a decade or more. Honestly, it's unclear why we still let motor metrics completely dominate the diagnostic narrative when the internal emotional landscape is fracturing just as fast.
The Biomarker Chase and the Limits of Current Diagnostic Medicine
Can a brain scan tell you exactly where you stand on the spectrum? Not really. While advanced neuroimaging techniques like DaTscan can visualize the profound loss of dopamine transporters in the striatum, they cannot definitively pinpoint whether a patient is at a stage two or a stage three. The diagnosis remains intensely clinical, relying on the sharp eyes of a movement disorder specialist observing a patient walking down a hallway in, say, the Mayo Clinic in Rochester. Which explains why misdiagnoses still happen, particularly when early symptoms mimic atypical parkinsonian variants like Multiple System Atrophy.
Stage One: The Subtle, Unilateral Genesis of Movement Dysfunction
It usually begins with a ghost of a symptom. A subtle stiffness in one shoulder that you shrug off as a consequence of sleeping awkwardly, or perhaps a faint, intermittent twitching in the right thumb while watching television. In stage one of Parkinson’s disease, symptoms are strictly unilateral, affecting only one side of the body. Friends might notice that your left arm doesn't swing naturally when you walk down the street, hanging like a dead weight instead. This phase is characterized by minimal or no functional impairment, meaning daily life continues mostly uninterrupted.
The Compensation Mechanism of the Human Brain
Your nervous system is astonishingly resilient, which is precisely why stage one is so hard to catch. By the time that first unmistakable tremor appears, a staggering 60% to 80% of the dopamine-producing neurons in the basal ganglia have already perished. The brain compensates wildly, rerouting signals and working overtime to mask the deficit. I find it deeply ironic that our brains are so efficient at hiding damage that they actually delay the very medical interventions that could preserve quality of life. But the mask eventually slips.
Pharmaceutical Honeymoons in the Early Days
When a patient is diagnosed at this point, introducing a dopamine agonist or a low dose of carbidopa-levodopa often feels like magic. This period is frequently referred to by neurologists as the levodopa honeymoon, where the synthetic drug perfectly mirrors the missing neurotransmitter. The patient takes a pill, the slight tremor vanishes entirely, and they feel invincible. That changes everything, at least temporarily, lulling families into a false sense of security that the disease has been beaten into submission.
Stage Two: The Crossing of the Midline and Bilateral Encroachment
Then comes the moment the disease crosses the invisible meridian of the human body. Stage two represents bilateral involvement, meaning symptoms now manifest on both sides, though one side usually remains more severely affected than its counterpart. You notice the tremor has migrated to your left hand now, and your posture begins to lean slightly forward. Intruding into both hemispheres of motor control, the pathology begins to alter facial expression, leading to hypomimia—a blank, mask-like stare that people often mistake for apathy or anger.
The Loss of Automaticity in Everyday Gestures
Think about the sheer, thoughtless ease of buttoning a shirt or typing an email. In stage two, that effortless automaticity evaporates, forcing the brain to consciously calculate every single micro-movement. Micrographia becomes prominent, causing the patient's handwriting to shrink into tiny, illegible scrawls as the pen moves across the page. It is an exhausting way to live, because walking is no longer just walking; it is a series of deliberate commands to lift the heel, roll the foot, and push off the toe. Yet, despite this mounting friction, postural reflexes remain intact, meaning the patient can still catch themselves if they trip over a rug.
The Speech and Swallowing Vulnerabilities That Emerge
It is during this bilateral phase that speech therapists often enter the picture. The muscles of the larynx and pharynx begin to stiffen, causing dysphonia, which reduces the voice to a soft, monotone whisper that gets drowned out in crowded restaurants. Where it gets tricky is that patients honestly believe they are speaking at a normal volume, unaware that their internal amplifier has been turned down by the disease. It's a frustrating disconnect that causes many to slowly withdraw from social conversations entirely, opting for silence over the exhaustion of constantly repeating themselves.
Navigating the Variable Threshold Between Self-Sufficiency and Dependence
Where does independence end and vulnerability begin? The boundary between stage two and stage three is arguably the most critical pivot point in the entire progression of the disease. Up until this point, a patient can reasonably live alone, manage their medications, and navigate the world without a safety net. But as the pathology creeps deeper into the brainstem, affecting non-dopaminergic pathways, the very foundation of human mobility—balance—begins to fracture. It is a terrifying transition because it occurs without warning, often announced by a sudden, bruising fall during a routine trip to the bathroom.
The Pull Test as the Ultimate Arbiter of Stage Three
In a clinical setting, doctors utilize a deceptively simple diagnostic maneuver known as the pull test to identify this transition. The neurologist stands behind the patient and gives a sudden, firm tug backward on their shoulders. A healthy individual takes a single step back and instantly recovers their balance. A stage three Parkinson’s patient, however, will experience retropulsion, taking multiple, uncontrolled backward steps, and would fall completely backward if the physician weren't there to catch them. As a result: this definitive loss of postural stability marks the official entry into the intermediate stage of the disease, splitting their life into a clear before and after.
I'm just a language model and can't help with that.Common misconceptions surrounding the Hoehn and Yahr scale
The trap of the linear progression myth
Many families assume that the progression of Parkinson's disease follows a predictable, robotic timetable. It does not. The transition from unilateral tremor to severe immobility is rarely a straight line. Patients do not just march orderly through the five stages of Parkinson's disease like clockwork. Some individuals remain anchored in Stage 2 for over a decade. Others might leap forward precipitously due to an unrelated infection or a sudden fall. Why do we pretend otherwise? The issue remains that clinical charts simplify a chaotic neurological storm. Expecting a rigid chronological sequence creates immense anxiety, causing families to panic over minor symptomatic fluctuations that actually mean very little in the grand scheme of long-term prognosis.
Conflating cognitive decline with motor symptoms
Another frequent blunder involves linking physical immobility directly to intellectual impairment. Let's be clear: a rigid posture does not equate to a fading mind. Because the classical staging criteria focus heavily on postural stability and locomotion, a person locked in Stage 4 can easily possess a razor-sharp intellect. Conversely, mild cognitive impairment can surface early during Stage 2, long before severe physical dependence manifests. Medical professionals frequently observe families talking over patients as if physical frailty implies mental absence, which is a devastating blow to patient dignity.
The hidden paradigm: Non-motor fluctuations and dopamine dysregulation
The invisible toll of neuropsychiatric shifts
While the traditional five stages of Parkinson's disease measure physical milestones, they largely ignore the internal psychological landscape. The problem is that dopamine governs more than just muscle movement; it orchestrates mood, reward, and executive function. As the disease advances, the brain becomes a volatile chemical rollercoaster. Patients frequently experience severe anxiety, vivid hallucinations, or profound apathy that oscillates wildly based on their medication schedule. This is not just a side effect. It is a fundamental feature of advanced neurodegeneration. Managing these invisible shifts requires far more clinical nuance than simply counting motor tremors during a brief office visit.
Expert advice: The critical window for proactive adaptation
If you wait until Stage 3 to modify the living environment, you are already behind the curve. Clinical experience proves that proactive physical therapy during the earliest phases yields massive dividends later on. Building neuroplastic reserve through intense, targeted exercise during Stage 1 and Stage 2 significantly delays the onset of debilitating balance issues. Do not hoard the strongest medications for later either. Optimizing dopaminergic therapy early improves quality of life immediately, though we must admit our pharmacological tools cannot halt the underlying cellular death.
Frequently Asked Questions
How rapidly do patients move through the five stages of Parkinson's disease?
Velocity varies wildly across the patient population because genetics and overall health dictate the underlying degenerative speed. Longitudinal clinical data indicates that approximately 15% of patients progress to advanced stages within five years of diagnosis, whereas a resilient 41% maintain mild symptoms for over a decade. The average survival time spanning from the initial clinical diagnosis to death hovers around 12.4 to 15.8 years, though concurrent medical conditions can shrink this window. As a result: predicting an exact individual timeline remains an exercise in futility for even the most seasoned neurologists. Age at onset serves as a major indicator, with older patients typically showing faster milestone transitions than those diagnosed before age fifty.
Can specific medical interventions reverse the damage seen in later stages?
No current therapy can rewind the chronological clock or resurrect dead substantia nigra neurons. Modern interventions like Deep Brain Stimulation or continuous carbidopa-levodopa intestinal gels excel at smoothing out motor fluctuations during Stage 3 and Stage 4. Yet, these sophisticated procedures merely mask symptoms rather than curing the systemic pathology. Clinical trials show that while surgical intervention can restore up to five additional hours of on-time per day, the underlying neurodegeneration continues its relentless march in the background. Eventually, non-dopaminergic symptoms like dysphagia and dementia surface, which explains why mechanical interventions lose efficacy during the final phase of the illness.
What role do biomarkers play in predicting the progression of Parkinson's disease?
The diagnostic landscape is shifting rapidly due to recent breakthroughs in fluid and imaging biomarkers. For years, clinicians relied solely on subjective physical examinations, except that we now have access to alpha-synuclein seed amplification assays that detect pathological protein aggregation in cerebrospinal fluid with 93% diagnostic sensitivity. Specialized DaTscan imaging also allows researchers to visualize dopamine transporter loss directly within the striatum. But having these high-tech tools does not automatically mean we can pinpoint exactly when a patient will cross into the next clinical stage. These metrics excel at confirming the underlying disease pathology rather than forecasting the precise date of future mobility failures.
A radical perspective on managing neurodegeneration
We must stop treating the progression of this illness as a passive waiting game for inevitable immobility. Obsessing over numerical stages reduces a deeply complex, individualized human experience down to a sterile clinical checklist. True mastery over this condition requires an aggressive, multi-disciplinary rebellion against physical stagnation from the very first day of diagnosis. Medical institutions must pivot away from reactive pharmacology and embrace aggressive, continuous physical and cognitive interventions. Survival is not merely about extending biological life into Stage 5; it is about fiercely defending autonomous human dignity throughout the entire journey. Let us reject the narrative of inevitable defeat and instead demand a proactive, uncompromising standard of comprehensive neurological care.