Understanding the Vascular Volcano: What Happens When an Aneurysm Meets Thin Blood?
An aneurysm is not a clot problem. It is a structural failure, a localized ballooning of an artery wall where the structural integrity of the vessel has completely degraded. Think of a tire with a weak spot where the inner tube starts pushing through the rubber tread. When you introduce medications like warfarin, rivaroxaban, or plain old aspirin into this equation, you are not fixing the rubber. You are merely making the fluid inside less likely to clump. Intracranial aneurysms affect roughly 3% of the global population, sitting silently like ticking time bombs in the Circle of Willis at the base of the brain.
The Hemodynamic Nightmare
Where it gets tricky is the shear stress. Blood rushing through a weakened artery exerts a constant, pounding physical force against that thin tissue. If that wall gives way, the body’s instinctive survival mechanism is to form a rapid clot to plug the leak. But what if you have wiped out that mechanism with heavy anticoagulants? The bleeding does not stop. A normal micro-bleed that the body might have contained suddenly turns into a massive, catastrophic subarachnoid hemorrhage. It is a terrifying prospect, honestly, because the mortality rate for a ruptured brain aneurysm crawls up near 50 percent within the first thirty days post-rupture.
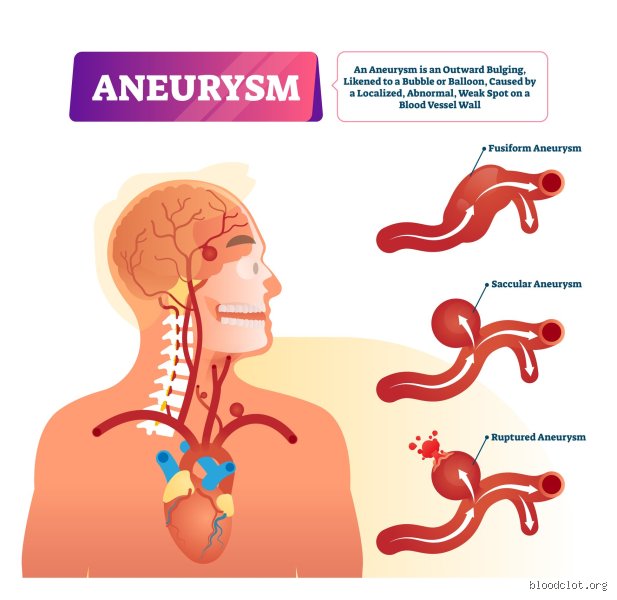
Why the Type of Bulge Matters
We cannot lump all vascular bulges into the same basket. An abdominal aortic aneurysm—frequently discovered by chance during routine ultrasounds in older smokers—behaves very differently from a tiny, berry-shaped blister in a cerebral artery. But the core physics remains unyielding. Except that with the aorta, the body's largest pipeline, a rupture means internal bleeding so rapid that survival becomes a matter of literal minutes, regardless of whether your blood is thin or thick.
The Paradoxical Protocol: When Specialists Deliberately Thin Your Blood
Now, let us flip the script completely because here is where conventional wisdom gets stood on its head. There are moments when a neurovascular surgeon will actively prescribe antiplatelet or anticoagulant agents to a patient with an unruptured aneurysm. Sounds insane? It isn't. This usually happens right after an endovascular coiling or stenting procedure, such as the deployment of a Pipeline Flex embolization device to divert blood flow away from the bulge.
[Image of endovascular coiling for aneurysm]Preventing Ischemic Stroke on Foreign Metal
The human body hates foreign objects inside its plumbing. When a surgeon slides a metallic mesh stent across the neck of a cerebral aneurysm, the blood cells immediately want to stick to that shiny new scaffolding. If they do, a massive clot forms, blocks the main artery, and causes a devastating ischemic stroke. To prevent this disaster, patients are placed on dual antiplatelet therapy—usually a combination of aspirin and clopidogrel—for at least 6 to 12 months post-procedure. So, does a blood thinner help aneurysms here? Indirectly, yes, because it keeps the cure from killing the patient, even though the inherent risk of a hemorrhagic bleed remains a shadow in the room.
The Micro-Clot Dilemma Inside the Sack
Sometimes, blood swirling inside that stagnant aneurysm sack naturally starts to solidify. You might think that is a good thing, right? A solid clot filling the balloon should stabilize it. But people don't think about this enough: those ragged micro-clots can break loose, travel downstream, and plug up smaller vessels feeding vital brain tissue. I have seen cases where a patient presenting with transient ischemic attacks was actually throwing tiny emboli from the depths of an untreated giant aneurysm. In those rare, highly debated instances, a delicate balance must be struck using low-dose therapy to stop the strokes without blowing up the artery.
Weighing the Collateral Damage: Clinical Data and Real-World Fallouts
Medical registries give us the cold, hard numbers on this gamble. Data from the International Study of Unruptured Intracranial Aneurysms (ISUIA) indicated that size is the ultimate predictor of danger, but concurrent use of anticoagulants adds a volatile wild card to the metrics. If you have a bulge larger than 7 millimeters in diameter, your baseline rupture risk is already elevated. Add a daily regimen of Eliquis or Coumadin for an unrelated condition like atrial fibrillation, and you have just supercharged the lethality of any potential leak.
The Atrial Fibrillation Conundrum
This is the classic medical catch-22 that keeps cardiologists and neurosurgeons arguing during morning rounds. An elderly patient has an irregular heartbeat that threatens to send a clot to the brain, requiring aggressive anticoagulation. But their routine MRI just revealed a 5mm unruptured aneurysm. What do you do? If you stop the blood thinner, they stroke out from the heart condition; if you keep it going, their brain might bleed. Experts disagree constantly on the exact threshold for intervention here, proving that standard guidelines look great on paper but often fail at the bedside.
The Alternative Frontier: Securing the Vessel Without Thinning the Blood
Because managing blood thinners around a vascular weak spot is like juggling live grenades, the medical tech world has sprinted toward solutions that eliminate the need for long-term drug regimens. The goal is simple: seal off the danger zone permanently so the patient can take whatever heart medications they need without terrifying side effects.
Surgical Clipping Over Endovascular Sleeves
The old-school method remains the gold standard for a reason. Microsurgical clipping involves a craniotomy—temporarily removing a piece of the skull—and placing a tiny titanium clip across the neck of the bulge. Once that clip snaps shut, the aneurysm is completely obliterated from the circulation system. The beauty of this invasive approach? It requires zero long-term antiplatelet therapy afterward. That changes everything for a patient who absolutely must stay on heavy blood thinners for a mechanical heart valve or recurrent deep vein thrombosis.
Common mistakes and dangerous misconceptions
The "clot is a clot" fallacy
People often conflate ischemic strokes with hemorrhagic events. They assume that because blood thinners prevent clots in the heart, they must magically stabilize every vascular anomaly. They do not. Anticoagulants do not dissolve the structural weakness of an arterial bulge. In fact, if you introduce these aggressive agents into a system with an undiagnosed, fragile vascular wall, you are essentially pouring gasoline on a hidden spark. The problem is that a thinning agent reduces the blood's ability to plug a microscopic tear. One tiny fissure becomes a catastrophic subarachnoid hemorrhage within minutes. Why do we keep seeing patients self-medicate with leftover aspirin when they feel pulsing headaches? It is a terrifying gamble driven by internet pharmacology.
Assuming all aneurysms are treated equally
Location dictates the entire medical playbook. An unruptured abdominal aortic aneurysm has an entirely different hemodynamic profile compared to a tiny berry aneurysm nestled in the circle of Willis. Yet, patients frequently browse online forums and assume a protocol for a leg clot applies to their brain. Let's be clear: blood thinners can actively destabilize intracranial aneurysms by altering the shear stress of blood flow against the weakened dome. Because the structural integrity of the vessel wall is already compromised, thinning the fluid increases the kinetic impact of every single heartbeat. Except that people ignore this fluid dynamic reality, preferring to believe a single pill fixes all circulatory woes.
The hidden hemodynamic paradox: Expert insights
The turbulent vortex phenomenon
Medical students are taught that stasis breeds clots. Inside a ballooning artery, blood swirls in a sluggish, chaotic vortex. You might think preventing a clot there is helpful, right? Wrong. In many cases, a small, controlled intra-aneurysmal thrombus actually stabilizes the structure by thickeneing the wall from the inside. Anticoagulation therapies disrupt this natural scaffolding. By melting away this accidental protective lining, the drug exposes the raw, paper-thin arterial tissue to maximum pressure. It is a delicate balancing act that leaves even veteran neurosurgeons sweating during clinical decisions.
When the rule book gets thrown out
But what happens when a patient absolutely needs these drugs for a mechanical heart valve, yet harbors a ticking vascular time bomb in their head? This is the ultimate clinical tightrope. We must weigh the immediate risk of a cardiac embolic stroke against the statistical probability of an aneurysmal blowout. As a result: physicians utilize advanced flow-diverting stents to physically isolate the bulge before they dare touch a prescription pad. (This dual-therapy approach requires daily monitoring of platelet inhibition levels). Does blood thinner help aneurysms in this specific scenario? No, it complicates the treatment exponentially, forcing us to use hardware to protect the patient from the very medication saving their heart.
Frequently Asked Questions
Can taking daily aspirin cause an unruptured brain aneurysm to leak?
Clinical data from global vascular registries indicate that a standard 81 mg low-dose aspirin regimen does not significantly increase the rupture rate of small, stable intracranial aneurysms under 5 millimeters. However, the risk landscape shifts dramatically if the structural defect exceeds a critical 7-millimeter threshold where wall tension is inherently higher. In those larger anomalies, unmonitored antiplatelet use can exacerbate micro-bleeds and hinder the body's localized clotting defenses. Which explains why a comprehensive digital subtraction angiography is mandatory before initiating long-term therapy. You cannot guess safety margins when dealing with intracranial pressure dynamics.
What should you do if you need anticoagulants for atrial fibrillation but have an aneurysm?
This scenario requires immediate, multidisciplinary intervention involving a cardiologist and a neurovascular specialist to calculate your precise CHA2DS2-VASc score against your specific rupture probability percentage. If the stroke risk from atrial fibrillation exceeds the bleeding risk of a stable, coiled anomaly, therapy may proceed under strict blood pressure parameters. Often, teams will choose a left atrial appendage closure device to eliminate the need for systemic anticoagulants altogether. The issue remains that every patient possesses a unique vascular architecture that defies generalized guidelines. Have you discussed these overlapping risks with a certified stroke team yet?
How do doctors safely manage blood clots in patients who also possess known arterial bulges?
Physicians navigate this nightmare by utilizing targeted, short-acting intravenous medications like heparin rather than irreversible oral anticoagulants. This allows the clinical team to instantly deactivate the thinning effect within a precise 90-minute clearance window if imaging shows structural destabilization. Furthermore, endovascular interventionists might deploy a temporary inferior vena cava filter to catch migrating clots mechanically without altering blood chemistry. It is a high-tech game of biological chess. Ultimately, the priority is always protecting the brain first, even if it means tolerating minor peripheral clots temporarily.
A definitive medical stance on vascular management
We must stop treating systemic circulatory drugs like harmless, all-purpose tonics. The clinical truth is brutal: standard anticoagulation profiles are fundamentally hostile to weakened arterial walls. Does blood thinner help aneurysms? Absolutely not; they represent an adversarial force in structural vascular disease. We recognize our therapeutic limits, acknowledging that we cannot perfectly predict when a vessel wall will yield to hemodynamic stress. Yet, prescribing these aggressive agents to a patient with an unprotected arterial bulge is a game of medical Russian roulette. True vascular health requires precise mechanical interventions, not a blanket reliance on chemical thinning. We must prioritize structural reinforcement over pharmaceutical shortcuts every single time.